Anxiety may be the scourge of our times, but it now appears we have “scanxiety”, too. According to a study of 2,000 women, the phenomenon of pregnant women paying for extra private scans is on the rise. Almost a third paid for scans during pregnancy, with 36% citing anxiety as a reason. The NHS offers routine scans at 12 and 20 weeks, although more may be given for medical reasons.
“For the last 20 years, it’s been quite common for women to access private facilities for scans,” says Dr Christoph Lees, a consultant in foetal and maternal medicine and obstetrics and a spokesman for the Royal College of Obstetricians and Gynaecologists. “Sometimes it’s simply for reassurance, or because they don’t feel they’re getting sufficient scans on the NHS. Sometimes they’re accessing a service that isn’t routinely provided, such as 3D and 4D scans. Many are what you might call souvenir scans.”
For Lauren McGlynn, who has two boys aged four and nine months, anxiety was the main reason for paying for private scans. “Before my first son, I had two miscarriages,” she says. “I just couldn’t deal with waiting until 12 weeks. I had a private scan at seven weeks, which is the earliest they will let you do it.” Did she speak to her midwife or doctor about her worries and ask for an early scan on the NHS? “I didn’t say anything,” she says. “I just assumed the NHS wouldn’t be able to give an extra scan to every woman who had a miscarriage.”
Mandy Forrester of the Royal College of Midwives believes the rise may be partly explained by the shortage of 3,500 midwives in England (Lees also points to the national shortage of sonographers). “Midwives are pressurised during antenatal appointments and continuity of care is an issue,” she says. “If a woman is seeing the same midwife, it’s more likely they will build a good relationship. It may be that women are not getting the reassurance they need.”
There is also the issue of the small, unconfirmed risk to the foetus associated with ultrasound, which is why multiple scans without sufficient medical reason are not recommended. “And it’s difficult to know the quality of the service,” Lees adds. “While there are many private providers that are extremely good, there are pop-up services where the person doing the scan doesn’t have any training in ultrasound. You don’t need to have a licence to do an ultrasound scan privately.” Does he often see women who have had private scans that have worried them? “I do see women who come back to me with a private scan report,” he replies. “Quite often we have to repeat the scan and sometimes the advice is not correct. [Private scans] can cause concerns that are not necessarily merited, which rather negates their point.”
A right-wing hero was born this past Sunday during the combination bikini contest and civics test that is the Miss USA pageant. In an effort to probe how she’d solve our nation’s problems, host Julianne Hough asked Miss Washington DC (aka Kara McCullough) if she believed “affordable healthcare for all US citizens” was “a right or a privilege,” and why. McCullough answered by saying:
“I’m definitely going to say it’s a privilege. As a government employee, I’m granted healthcare and I see firsthand that for one to have healthcare, you need to have jobs. So therefore, we need to continue to cultivate this environment that we’re given the opportunity to have healthcare as well as jobs to all American citizens worldwide.”
Currently unemployed people, as well as those with bad jobs that don’t provide healthcare, are presumably out of luck. That McCullough wants to help women find work in Stem jobs is admirable, but does nothing to help the vast majority of people.
Of course, her statement is technically true. As things currently stand in the US, healthcare is a privilege, and one you likely need a job to access. (And not just any job … a salaried and/or union one, a holy grail that’s fast disappearing.) As a person with both a job and healthcare, she’s observed this firsthand. But as Ms McCullough is a nuclear scientist, I will assume she understood the question was about how she believes things should be, not how they are. In which case, she’s as wrong and out of touch as any DC royalty currently making policy on this issue.
Now, I’ll admit it’s tough to prove beyond the shadow of a doubt that people deserve basic levels of physical safety simply by virtue of being human. To do so would require a philosophical deep dive above my level of expertise. But our founding documents — which I’d hope someone with the surname “USA” respects — have already sided with the “yeas” on the existence of certain inalienable rights, chief among them “life.” And an estimated 45,000 Americans die each year from lack of health insurance. This is not just another commodity, but a necessity on the level with food and shelter. Which, to be fair, Republicans also want to take away from the poor.
Beyond that, it comes down to a simple matter of preference: do you want to live in a society that codifies some level of responsibility to our fellow citizens, or would you rather roll the dice on a Randian dystopia where the lazy, unlucky or otherwise uncompetitive are liquefied into paleo shakes for rich people? Maybe I can’t objectively prove which is “better,” but I know which I’d prefer. Contrary to what social Darwinists would tell you, one cool thing about being human is we (theoretically) get to decide which ideals we want to pursue.
When healthcare is a for-profit enterprise, costs skyrocket and access plummets. While the Affordable Care Act reined in some of the industry’s worst abuses, an estimated 27 million are left uninsured under it, a number that’s slowly climbing as companies raise premiums and pull out of exchanges.
Even those who are insured report problems paying for care due to high deductibles, and, more generally, to being insured by companies whose business model is to dole out as little coverage as they can legally get away with. The Republican party is currently in the process of turning 27 million into 52 million with their ironically named “American Healthcare Act.” Soon, 45,000 deaths a year will seem like the good old days.
As every other country in the developed world knows, the only way to increase coverage to 100% — as well rein in absurdly high per capita spending on a bloated private industry — is with a system of state-funded healthcare. It works everywhere else, and many experts say it would work here.
The American people are on board. A 2017 Economist/YouGov poll found about 80% of Democrats and 40% of Republicans — yes, Republicans! — favor a federally funded health insurance system that covers all Americans. All race, age, income, and gender demographics favor it by simple majorities, and many — particularly the most marginalized — by strong ones. Even Republicans and conservatives approach 50%. Those who voted for Hillary Clinton favor it at a rate of some 85%.
Unfortunately, this is one of many areas where the country’s political class refuses to even remotely entertain the will of the people. Neither Democrats nor Republicans are willing to do the empathetic, fiscally responsible thing.
We all know Republicans will happily let people die to pay for oligarchs’ tax breaks. But even most elected Democrats remain irrationally committed to compromising with an industry that wants you dead. This becomes more comprehensible when you look at the amount of money the insurance lobby gives to both parties. Despite its immense popularity with voters, single-payer will be on neither party’s agenda in 2018.
In stating that affordable healthcare is a privilege that should be reserved for gainfully employed people, McCullough showed she’ll fit in just fine with the other undemocratically elected rulers in DC. President Trump might not own the Miss USA pageant anymore, but his cutthroat spirit lives on.
Omid, a 54-year-old man who lives and works in London, was diagnosed with multiple system atrophy in 2014, a condition that cannot be cured and affects the nervous system. He has a wife and children but rarely sees them in order to spare them the agony. He attempted suicide in 2015 and was then moved to a nursing home. Even with care and family support, Omid wants to die to relieve his suffering. The alternative is to seek assistance to die abroad, but this will cost £10,000-£14,000, and he can’t afford this.
Omid wants to change the assisted dying law in England and Wales – a courageous and selfless act considering his condition. He wants to help others and to leave a legacy. The current law, although it does not criminalise suicide, forbids helping or encouraging suicide.
Omid argues that the law violates his right to private life, in breach of the Human Rights Act. The law does not allow him, and other competent and informed people in his situation, to choose how and when to die. He wants the high court to declare the law incompatible with the concept of human rights.
Rather than being terminally ill Omid has several years to live in this unbearable condition. Previous, failed attempts to change the assisted dying law, by Lord Falconer and Rob Marris, restricted assisted dying to terminally ill people with six months to live. This is a crucial difference with the current, ongoing Noel Conway case. Omid is asking for a change of the law for those with incurable conditions who may have many years of misery and pain ahead. The passing of an assisted dying law for terminally ill people would not have helped him.
The most recent right-to-die case in the UK involved Tony Nicklinson and Paul Lamb in 2014. A majority of judges (5-4) in the supreme court said that, although the court could make a declaration that the law on assisted dying was incompatible with the concept of human rights, they would allow parliament the opportunity to debate the issue first.
Parliament has recently considered the law on two occasions: in 2013, Lord Falconer’s bill proposed that terminally ill, competent adults should be allowed to request and receive assistance in dying after approval by two doctors. The bill did not have enough time for a full review in parliament, but in any case, would have been too narrow to help Omid who has an incurable, yet non-terminal condition.
Rob Marris’s bill was hastily defeated by the House of Commons on 11 September 2015 by 330 to 118 votes. Many found the debate unimpressive, raising questions as to whether parliament is the right forum for such legally complex and morally charged questions.
The main arguments against Omid’s case are that it will lead to a “slippery slope” (for instance, assisted dying leading to the legalisation of euthanasia) and that it will make weak and vulnerable people susceptible to harm. But there is no evidence from other countries that problems of this sort have occurred. It would not be difficult to devise a system that makes sure that the system is not abused – for example by having two independent doctors certify that the decision is freely made and without pressure from relatives.
The courts have tried to duck out of the responsibility once for not making the decision – they cannot afford to do it again if society is to have confidence in the legal system. The pain and misery this is causing is unbearable for people like Omid. They require and deserve the protection of the courts. The time has come for a change in the law.
Infertile mice have given birth to healthy pups after having their fertility restored with ovary implants made with a 3D printer.
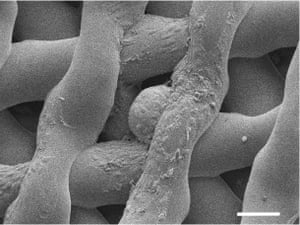
Researchers created the synthetic ovaries by printing porous scaffolds from a gelatin ink and filling them with follicles, the tiny, fluid-holding sacs that contain immature egg cells.
In tests on mice that had one ovary surgically removed, scientists found that the implants hooked up to the blood supply within a week and went on to release eggs naturally through the pores built into the gelatin structures.
The work marks a step towards making artificial ovaries for young women whose reproductive systems have been damaged by cancer treatments, leaving them infertile or with hormone imbalances that require them to take regular hormone-boosting drugs.
“Our hope is that one day this ovarian bioprosthesis is really the ovary of the future,” said Teresa Woodruff at Northwestern University in Chicago. “The goal of the project is to be able to restore fertility and endocrine health to young cancer patients who have been sterilised by their cancer treatment.”
[embedded content]
Of seven mice that mated after receiving the artificial ovaries, three gave birth to pups that had developed from eggs released by the implants. The mice fed normally on their mother’s milk and went on to have healthy litters of their own later in life.
Writing in the journal Nature Communications, the scientists describe how they printed layered lattices of gelatin strips to make the ovary implants. The sizes and positions of the holes in the structures were carefully controlled to hold dozens of follicles and allow blood vessels to connect to the implants. Mature eggs were then released from the implants as happens in normal ovulation.
Chemotherapy and high doses of radiation used in cancer treatment can destroy some or all of a woman’s eggs, putting them at risk of infertility and an early menopause. And while doctors have had some success in restoring women’s fertility from frozen ovarian tissue, an implant could potentially help those who do not bank healthy tissue when they are children.
Monica Laronda, a co-author on the study, said that an ovary implant could also help cancer survivors whose eggs are so damaged that they need hormone replacement therapy to trigger puberty. “We’re thinking big picture, meaning every stage of the girl’s life, so puberty through adulthood to a natural menopause,” she said.
A microscopic image of an immature mouse egg, surrounded by supportive cells, after it has been housed in a bioprosthetic ovary scaffold for six days. Photograph: Northwestern University
Scientists have made artificial ovaries for mice before, but the latest research is believed to be the first time that researchers have used 3D printing to manufacture them. It is not clear if the same approach will work in people because human follicles are much larger and grow rapidly until they are visible to the naked eye.
Other animal experiments performed nearly a decade ago hinted that women who had ovarian tissue transplants later in life might enjoy broader benefits from the procedure than restored fertility. In 2010, scientists at Kato Ladies Clinic in Tokyo found that ovarian transplants extended the lives of old mice, and led older females, who were normally inactive, to seek out mates and have babies. The researchers conceded that far more work was needed to assess the effects in women.
Advances in 3D printing have already transformed some areas of medicine by allowing the doctors to make bespoke body parts that can be directly implanted into patients. Last year, South Korean surgeons printed a titanium heel bone for a man who had a tumour removed from his foot.
Meanwhile, researchers in North Carolina announced that they had made ears, jawbones and skeletal muscles by 3D printing structures laced with living cells. Other groups have printed vascular networks that will be vital for creating large synthetic organs in the lab.
Labour’s 2017 general election manifesto is a big break with the recent past. Whether the manifesto allows the party to make a fresh connection with the British electorate won’t be clear until 9 June. What is beyond doubt is that this manifesto proclaims that politics and government in Britain do not have to be done in the way the country has long been accustomed to. That is true, and Labour is offering the country a real choice. So far, so very good, on both counts.
Jeremy Corbyn’s biggest achievement is to put several propositions back into the arena that had been thought extinct. That does not mean all of them deserve a new lease of life equally. Nationalisation in the shape of expensive, centralised public ownership is one to treat with caution, not least because of the power it gives to trade union leaders to drive up costs. There are signs that Labour’s economic team recognises that, but not enough detail about how it can be done. Other changes, though, are more straightforwardly welcome. The most important of these concerns taxation.
For 30 years or more, taking its cue from America, British politics took it as axiomatic that all voters will always recoil from increased taxes. Understandable though this was in some ways, it was a denial of the principle of social responsibility. As a result, throughout this era, parties have had to contrive ways of providing good levels of public provision without overt tax increases. Not surprisingly, this has become increasingly hard to maintain, and the effect on public goods has often been brutal. The no-tax assumption reached its nadir in 2015 when David Cameron and George Osborne promised no rises in income tax, VAT or national insurance for all. But it was an unachievable fantasy, as Philip Hammond found in the recent budget.
Labour is right to level with voters that tax rates cannot be set in stone for ever. Governments must be able to respond to economic changes, and those that want to invest in new programmes or projects must either borrow or tax to do so. Labour proposes to do both, which may alarm some voters. But the principle that fair and necessary taxes are a mark of a civilised society is the right one, and voters understand that they must rise as well as fall. Too few parties have been honest about this in recent times – the Liberal Democrats are an exception. Today it is not just Labour that is striding boldly into this territory. Even the Conservatives see the point of keeping options open. But it is Labour that confronts the issues with welcome audacity.
The real question is whether Labour is proposing the right level of tax take and the right mix of taxes and spending. There is a discussion to be had here. Taxes on income are very important, but taxes on wealth, including houses and land, which are less easy for the asset-rich to avoid, do not get as much focus as they should. Labour’s boldness does not extend to uprating and reforming council tax bands, for instance; instead only a review into reform is promised. There is nothing in the manifesto about fuel or alcohol taxes, both of which raise money and have social dimensions too. Abolishing tuition fees is an expensive subsidy to the better-off.
It is possible that the election has simply come too quickly for Labour to work everything out properly here. Some of the changes that have been made to the leaked draft last week add to that impression, though politics is involved too. The section on Trident and Nato has been sharpened at Mr Corbyn’s expense. The earlier plan to halt NHS reforms has wisely been replaced by a review. Looked at overall, Labour’s manifesto is a mixed bag of pledges, with some strange inclusions and other surprising omissions. Though radical in some ways it is conservative in others. The section on union rights is detailed and extensive, but that on the future of the United Kingdom is perfunctory. There is not as much sense of the future as there should be.
At 124 pages, this is a long manifesto. But it is not a suicide note. In terms of its social democratic credentials, the 1983 manifesto it most resembles is that of the Liberal/SDP Alliance rather than Labour’s. Its achievement is to expand the limits of the thinkable in British politics. Its weakness is that it does too little to make the thinkable seem realistic and practical. That reflects Mr Corbyn’s preference for energising his own support rather than persuading those outside it. This manifesto may not win Mr Corbyn the general election, but it could cement his support within his party.
Last week amateur chefs everywhere were absorbing instructions on how to cut an avocado, after a post-brunch A&E influx of injuries sustained while trying to prepare the fruit (Pass notes No 3,853: Avocado hand, G2, 11 May). Now I hope the nation might broaden their knowledge further by learning how to help someone having an epileptic seizure. It’s National Epilepsy Week, and our new YouGov poll shows that two-thirds of UK adults with no experience of epilepsy would not know how to help. This is worrying when London Ambulance Service alone attends 40 epileptic seizures a day. Taking two minutes to read our seizure first aid steps – www.epilepsysociety.org.uk/10-first-aid-steps-for-convulsive-seizures – could make all the difference in a crisis. Clare Pelham Chief executive, Epilepsy Society
• Join the debate – email guardian.letters@theguardian.com
• Read more Guardian letters – click here to visit gu.com/letters
A teenager in the US died because he consumed too many high-caffeine drinks in a short space of time, a coroner has said.
Davis Allen Cripe died last month, about an hour after collapsing in his high school near Columbia, South Carolina. The 16-year-old had consumed a latte from McDonald’s, a large Mountain Dew drink and a highly caffeinated energy drink in just under two hours, Richland county coroner Gary Watts said.
Doctors said Davis died from a “caffeine-induced cardiac event causing a probable arrhythmia”, according to Watts.
He added that the teenager was considered healthy and the autopsy showed no sign of an existing undiagnosed heart condition.
“This is not a caffeine overdose,” said Watts. “We’re not saying that it was the total amount of caffeine in the system, it was just the way that it was ingested over that short period of time.”
Davis weighed about 90kg but would not have been considered morbidly obese, according to Watts, who added that he would have been unharmed by the same amount of caffeine on another day.
“We’re not trying to speak out totally against caffeine,” said Watts. “We believe people need to pay attention to their caffeine intake and how they do it, just as they do with alcohol or cigarettes.”
The particular energy drink Davis drank was not known but a witness said it was from a container the size of a large soft drink.
According to caffeineinformer.com, a McDonald’s latte has 142 milligrams of caffeine, a 20-ounce Mountain Dew has 90 mg, and a 16-ounce energy drink can have as much as 240 mg.
The US Food and Drug Administration and European Food Safety Authority both say that caffeine consumption of up to 400mg a day – about four or five coffees – is believed to be safe for adults. The EFSA says 200mg a day is safe for women who are pregnant or breastfeeding and that single doses of up to 200mg do not give rise to safety concerns. The American Academy of Pediatrics discourages the consumption of caffeine and other stimulants by children and teenagers.
Caffeine has been linked to previous deaths, although the cases are few and far between and the link not always clear-cut. In 2011, 14-year-old US schoolgirl Anais Fournier, who had a pre-existing heart condition, died after drinking two cans of Monster energy drink, containing a total of 480mg of caffeine. The company denied any responsibility.
In 2015, two students at Northumbria University, were were left fighting for their lives after they were accidentally given the equivalent of 300 cups of coffee in a botched experiment. They eventually made a full physical recovery.
Tony Heagerty, professor of medicine at Manchester University, said it was likely that Davis had a genetic heart condition, which may not have revealed itself in the autopsy, and that the caffeine put stress on his heart.
“I think the caffeine must have interacted with something wrong with this heart,” he said. “If you are an unfortunate person with a pre-existing condition and put yourself in a stressful situation by drinking too much caffeine you are in danger.”
But he said the levels consumed by Davis would not be harmful to the overwhelming majority of people, except for making them feel strange.
Mike Knapton, associate medical director at the British Heart Foundation, said: “It is well known that caffeine increases a person’s heart rate but it can also trigger more serious effects, including heart palpitations, in those who are more sensitive to caffeine.
“People with cardiac abnormalities, including inherited heart conditions, and those who drink toxic amounts of caffeine are more susceptible to the side-effects of caffeine. Tragic accidents like this are rare but, with increasingly strong coffees and caffeinated drinks on the market, moderation is key to monitoring your caffeine intake.”
Caffeine – what are the dangers?
The World Health Organisation recognises caffeine use disorder and caffeine dependence as illnesses.
Drinking large amounts of coffee can lead to unpleasant side-effects such as irritability, problems sleeping, restlessness, according to the NHS.
It can also result in babies having a low birth weight, which can increase the risk of health problems in later life, or miscarriage.
Caffeine constricts the coronary arteries, leading to a temporary rise in blood pressure. If drunk in sufficient quantities it causes calcium to be discharged from inside cells and causes the heart to beat faster. In the most extreme cases – caffeine toxicity – it causes major organs to shut down.
Symptoms of a caffeine overdose include dizziness, nausea, vomiting, convulsions and a high heart rate.
“Eurgh! This doll’s fat!” Those were the words of my five-year-old daughter and seven-year-old niece on encountering the Fashionistas range of new-size Barbies in a toyshop this weekend. To describe these dolls as “plus size” would be an exaggeration. But, given the emaciated state of regular Barbies, I can see what the fuss is about. These dolls look normal – and normal, in a Barbie context, looks decidedly weird.
I have to act. “See these Barbies,” I say, pointing at the more traditional ones. “They are really hungry. They haven’t had enough to eat. But these new Barbies” – I hold up a Fashionista – “feel much better. They’ve got strong legs, see?”
“Ohhhh,” one of them nods. I realise my explanation is not perfect: I don’t want these two telling skinnier children in the playground that they’re malnourished. But given that traditional Barbies represent the body shape of 1 in 100,000 real-life women, have a waist size 20cm smaller than a group of anorexia sufferers, and would have insufficient body fat to menstruate, I’ll take my chances.
There is no ideal way to counter the messages these impressionable young girls are absorbing about body image. I welcome the fact that Barbies now come in four body types and seven skin tones, and wear their hair in braids or Afros. Beyoncé’s stylist, Marni Senofonte, who designed those dolls, says: “I want a girl who is not necessarily small to say: ‘OK, I could wear a crop top, and I could wear jeans with big holes in and fishnets underneath it, and I am cute.’”
That’s great. But let’s not forget that the legacy of old Barbie – who in 1963 was released with a book entitled How to Lose Weight – looms large. So much so that when a five and seven year old – neither of whom have yet graduated on to being critical of their own bodies, thankfully – see a doll with a normal figure, their initial reaction was disgust.
The small world of Brexit
Theresa May greets Jean-Claude Juncker at 10 Downing Street. Photograph: Carl Court/Getty Images
There has been plenty of debate about the estimated rise in hate crime since the EU referendum, which ranges from 40% to 100%. But less often discussed is the impact of the vote on British people’s sense of identity.
A recent report suggests that this is widespread, and perhaps more enduring. It finds that, since the referendum, ethnic minorities in the UK are now less likely to identify as British, and more likely to claim the identity of their ethnic heritage instead.
White British people too are becoming less likely to embrace Britishness or other national identities, such as English or Scottish, and more likely to identify with their local area or community. They have, according to Opinium, “withdrawn from a wider sense of belonging to focusing in on the immediate world around them”. Long after the bickering of Theresa May and Jean-Claude Juncker, these injuries to our identity will remain.
Celebrity shares
Stormzy at the Brixton Academy. Photograph: PJP photos/Rex Features
Labour has now pledged in its manifesto to scrap university tuition fees in its manifesto launch todayyesterday. But if, as is widely predicted, the Tories win, fees are likely to rise above the current £9,000 a year; and as long as they do so, inevitable comparisons will continue to be made with the cost of study in the US, which currently averages a cool $ 33,000 (£26,000) a year at a private college.
If we are going to have US-style fees, we will need US style benefactors, made generous by US-style salaries, which are 50% higher than UK equivalents in some sectors.
In the meantime, celebrities have been stepping in. The UK rapper Stormzy this week became the latest to dip into his fortune, giving a final-year Oxford student £9,000 to do her master’s at Harvard. With some of the funding promises currently going around, I wouldn’t be surprised if sourcing donations from superstars appears somewhere as an election pledge.
The ransomware attack that disrupted the NHS and businesses around the world has led to a boom in share prices of cybersecurity companies – including the firm used by the health service to protect it against hackers.
With governments and companies expected to increase spending on IT security after being caught out by the attack, cybersecurity firms have seen their stock market values climb sharply over the past two days.
Sophos, a cloud network security specialist which counts the NHS among its clients, has seen its shares jump 8%. Over the weekend, a claim on the company’s website that “the NHS is totally protected with Sophos” was changed to “Sophos understands the security needs of the NHS”. Last week, Sophos tweeted its “top five tips for securing NHS organisations”. But its shares have been performing well over recent months because of the increased need for cyber defences.
Meanwhile, NCC group added 5% to its share valuation and cyber consultancy group ECSC surged 42%. ISE, a fund invested in cybersecurity businesses, added nearly 4%.
The surge has been put down to the attacks refocusing businesses on the need for adequate cybersecurity. “Significant increases in public sector cyber defence spending [are] now looking inevitable,” said Nicholas Hyett, equity analyst at Hargreaves Lansdown. “[Sophos] already provides services to the healthcare industry and will be looking to increase selling to the sector in the aftermath of the attack.”
US firms have also benefited, with FireEye’s prices rising 7%, Symantec up more than 3% and Palo Alto Networks 2.7% better. Neil Campling, head of technology research at financial services firm Northern Trust, told Reuters: “These attacks help focus the minds of chief technology officers across corporations to make sure security protocols are up to date, and you often see bookings growth at cybersecurity companies as a result.”
It was also suggested that the success of the WannaCry hack could make other attacks more likely in the future amid doubts over governments’ ability to secure “cyberweapons” from theft.
“The attacks raise significant questions about whether or not countries that are developing and stockpiling cyberweapons can do more to protect those tools from being stolen and turned against their own population,” said Thomas Fitzgerald, associate fund manager at EdenTree Investment Management. “The WannaCry attack is likely to be a catalyst for more of these types of cyber-attacks from copycat criminal organisations.”
The effects of the attack continued to be felt on Tuesday, although one of the seven NHS trusts which had still been experiencing serious problems on Monday, James Paget university hospitals trust in Norfolk, said that all of its operations and appointments were going ahead as scheduled.
Elsewhere the disruption continued. East and North Hertfordshire trust advised people to only go to A&E if absolutely essential.
Southport and Ormskirk hospital said it was continuing to experience difficulties with its clinical information systems but insisted that patient safety was being maintained. It advised all patients scheduled for surgery on Tuesday not to attend unless contacted and said all outpatients and endoscopy appointments were cancelled.
Barts health NHS trust said it was no longer diverting ambulances from its hospitals but was still experiencing delays and disruption. York teaching hospital NHS trust said bone scans at Scarborough hospital were not going ahead on Tuesday and that breast screening clinics in some areas had been cancelled. A number of affected trusts asked patients not to contact them by email because of ongoing IT problems.
NHS Digital said none of its services had been affected by the attack.
Businesses and NHS brace for fresh impact as minister blames Labour for UK’s cyber-security failings
Did you pay money as a victim of ransomware?
Russia had nothing to do with a massive global cyberattack, President Vladimir Putin said Monday, criticising the US intelligence community for creating the original software, AFP reports.
“As for the source of these threats, Microsoft’s leadership stated this directly, they said the source of the virus was the special services of the United States,” Putin said.
Three hospitals in Ireland have been targeted by the cyber attack.
Health chiefs blocked external communication to servers until Wednesday to stop the spread of the “ransomware” virus as officials confirmed that up to 20 computers had been affected.
The health secretary, Jeremy Hunt, has broken his silence on the cyber- attacks after pressure to comment.
He said there has not been a second wave of cyber attacks after the NHS was struck by ransomware attacks on Friday, PA reports.
Thousands of NHS computers were still using the old Windows XP operating system, the government has revealed, though a Number 10 spokesman insisted other Windows’ systems were also affected.
The prime minister’s spokesman said the NHS had updated the vast majority of its systems but just under 5% were still operating Windows XP.
Health trusts across England were sent details of an IT security patch that would have protected them from the crippling ransomware attack, NHS Digital said.
NHS Digital, the arms-length body of the Department of Health that provides information, data and IT systems for the NHS, said it had made health trusts aware last month of IT protection that could have prevented the attack.
The French government cyber security agency ANSII knows of “fewer than 10” French companies that have fallen victim to a global hacking attack that hit car factories, hospitals and other organisations in about 100 countries, an ANSII spokesman said on Monday.
The Prime Minister’s official spokesman has defended health secretary Jeremy Hunt’s lack of public statements or appearances since the cyberattack on Friday.
“This is an international cyber crime, committed on an unprecedented scale.
Theresa May has rejected claims the government ignored warnings the NHS was vulnerable to a possible cyber security attack.
The Prime Minister said warnings had been given to hospital trusts.
If you paid money as a victim of ransomware we’d like to hear from you. How much were you asked to pay? Why did you decide to pay the ransom? What happened afterwards? We’d also like to hear the experiences of those who paid in other recent attacks. You can share your stories with us – anonymously if you wish – by filling in our form here.
Few major problems have been reported in India with the hea of the government response team saying “everything seems to be normal, so far”, AP reports.
Experts estimated 5% of affected computers were in India, with the Computer Emergency Response Team of India issuing a red-colored “critical alert”.
Microsoft’s top lawyer has called on governments around the world to treat the international cyber attack as a “wake-up call” as he laid part of the blame at the door of the US administration, PA reports.
Brad Smith, the technology firm’s president and chief legal officer, criticised US intelligence agencies the CIA and the National Security Agency (NSA) for “stockpiling” software code which could be exploited by hackers.
“Hundreds of thousands” of Chinese computers at nearly 30,000 institutions including government agencies have been hit by the global ransomware attack, a leading Chinese security-software provider has said.
The enterprise-security division of Qihoo 360, one of China’s leading suppliers of anti-virus software, said 29,372 institutions ranging from government offices to universities, ATMs and hospitals had been “infected” by the outbreak as of late Saturday, AFP reports.
Blackpool Teaching Hospitals NHS Foundation Trust, NHS Blackpool Clinical Commissioning Group (CCG) and NHS Fylde and Wyre CCG are still experiencing some IT problems.
They said services are open and operating “as best as possible” but asked patients only to attend A&E in life-threatening and urgent cases.
The Royal Liverpool and Broadgreen University Hospitals Trust reported their IT system had not been attacked and was operating normally.
Likewise the Pennine Acute Hospitals NHS Trust, which runs hospitals in Manchester, Oldham and Rochdale, said they had not been affected by the attack but had taken precautionary measures to protect their IT systems.
The Southport and Ormskirk Hospital NHS Trust said patient safety is being “maintained” but difficulties are continuing.
Patients scheduled to have operations today have been asked not to attend hospital unless they have been contacted directly.
European governments and companies appeared early Monday to have avoided further fallout from a crippling global cyberattack, the police agency Europol said.
“The number of victims appears not to have gone up and so far the situation seems stable in Europe, which is a success,” senior spokesman for Europol, Jan Op Gen Oorth told AFP.
No patient data has been lost in the ransomware attack on Scottish NHS computer systems, Nicola Sturgeon has said.
Eleven health boards as well as NHS National Services and the Scottish Ambulance Service were affected Friday’s attack, PA reports.
Foreign Secretary Boris Johnson, arriving in Brussels for a meeting of EU foreign ministers, said the cyber-threat was not on the agenda.
He said: “Cyber-security is a huge issue for all of us in all our countries.
Three days on from the initial outbreak, fewer than a hundred victims of the WeCry malware appear to have given in and paid the ransom, according to analysis of the two bitcoin addresses to which the software demanded payment.
In order to restore encrypted files, the malware demands a payment of $ 300 in the cryptocurrency, sent to one of two addresses hardcoded into the software. Yet the contents of the addresses, which like all bitcoin wallets are publicly viewable, shows just under 14 bitcoin has been sent to them in total. At current exchange rates, that is worth slightly under $ 25,000, suggesting just 82 victims have paid the ransom.
Jeremy Hunt was warned last summer that the NHS was failing to prioritise cybersecurity and continued to use obsolete computer systems, the Times reported.
The Care Quality Commission and Dame Fiona Caldicott, the national data guardian, wrote to the health secretary to point out a worrying “lack of understanding of security issues” and that “the external cyberthreat is becoming a bigger consideration”.
York Teaching Hospital NHS Foundation Trust, which was hit by the attack on Friday, said some out-patient appointments had been cancelled on Monday – especially at Selby War Memorial Hospital – but most were not affected.
The trust said bone scan appoints had been cancelled in Scarborough and in Selby: “All outpatient appointments are cancelled except blood-taking and MSK physiotherapy.”
The British cybersecurity researcher described as an “accidental hero” for halting the global spread of the ransomware attack has spoken of his fears for his safety after a number of media outlets revealed his identity.
The 22-year-old, who tweets as @malwaretechblog, told the MailOnline: “In future someone might want to retaliate – they could find my identity within seconds.
Meanwhile in Japan, AP reports the ransomware attack hit computers at 600 locations but appeared to cause no major problems as Japanese started their workday Monday even as the attack caused chaos elsewhere.
Nissan Motor Co. confirmed some units had been targeted, but there was no major impact on its business.
As the UK wakes up on Monday braced for fresh impact as NHS returns to work, Chinese state media say more than 29,000 institutions across China have been infected by the global “ransomware” cyberattack, AP reports.
Xinhua News Agency reports that by Saturday evening, 29,372 institutions had been infected along with hundreds of thousands of devices. It cited the Threat Intelligence Center of Qihoo 360, a Chinese internet security services company.
Welcome to live coverage of the fallout from last Friday’s ransomware attack.
Ben Wallace, UK security minister has been on BBC Radio 4’s Today programme defending its record on investment in cyber-security.
• This is not targeted at the NHS, it’s an international attack, says Theresa May
• NHS England declares major incident after ransomware blocks access to patient records, internal phones and emails
More than half of Scotland’s health boards have been affected by a large-scale cyber attack on NHS computer systems. GP surgeries and dental surgeries were among some of the locations hit by the ransomware attack on IT networks, the Press Association reports.
NHS Lanarkshire said only those patients requiring emergency treatment should attend hospital while they dealt with the issue on Friday.
The Agence France-Presse news agency reports that, in Spain, employees at the telecom giant Telefónica were told to shut down their workstations immediately through megaphone announcements as the attack spread.
Forcepoint Security Labs said that “a major malicious email campaign” consisting of nearly 5m emails per hour was spreading the ransomware.
Some more quotes from the prime minister. She has told reporters:
I think what is important is that we have recognised that increasingly we need to be aware of the need to address cyber security issues, that’s why the National Cyber Security Centre has been set up. It is now able to work with the NHS to support the organisations concerned and to ensure that patient safety is protected.
After the prime minister said she was “not aware of any evidence that patient data has been compromised”, Ross Anderson, a professor of security engineering at Cambridge university, advises caution.
The NHS are saying that patient privacy hasn’t been compromised, but if significant numbers of hospitals have been negligently running unpatched computers for two months after the patch came out, how do they know?
Some more on that statement from the prime minister, Theresa May, who says:
We are aware that a number of NHS organisations have reported that they have suffered from a ransomware attack.
This is not targeted at the NHS, it’s an international attack and a number of countries and organisations have been affected.
There are reports around that as many as 40 NHS organisations have been hit by the cyber-attack. NHS Digital says it is not going to confirm the number until tomorrow.
The cyber-attack that has hit the NHS is part of a wider international attack, the prime minister Theresa May has confirmed.
She said there is no evidence that patient data had been compromised.
One expert who has worked closely with law enforcement says this would be seen as an attack on critical national infrastructure. He says investigators will be examining systems affected by the ransomware to see how badly they are affected and whether they, in turn, can or already have infected other computer systems connected to them.
He adds that the fear is that the ransonware cannot be broken and thus data and files infected are either lost or that the only way to get them back would be to pay the ransom, which would involve giving money to criminals.
One question arising from the attack on a sector of critical national infrastructure is whether the government has a policy on paying ransom to cyber hackers.
British government policy in the case of a terrorist attack or of the taking of a person hostage is clear: ransom will not be paid. But it is not clear if a policy exists for the 21st-century cyber equivalent. The lead agency dealing with the attack on the NHS is the National Cyber Security Centre, an arm of GCHQ.
The New York Times is reporting that 12 countries, including the UK, have been affected.
It reports that the attack struck “computers across a wide swath of Europe and Asia”, saying that Japan, Russia, Turkey, Vietnam and the Philippines are among those affected.
Prof Alan Woodward, a security expert from the University of Surrey, says the attackers appear to have taken advantage of a chink in the armour of Microsoft XP that was exposed in a recent leak of CIA hacking tools.
He says the problem may have been exacerbated because organisations have not updated their software with the fixes made available, or are using outdated versions.
From what we can see, it is a piece of ransomware called wanna decryptor. It goes by other names but it emerged in February 2017. Since then, it has been modified and there is evidence that it is spreading using a flaw in the Microsoft network protocol called SMB, which was exposed in the recent dump of exploits that were allegedly from US intelligence agencies.
It is not just the NHS affected: reports suggest it is a global problem. The virulence is likely to be because some organisations have either not applied the patch released by Microsoft, or they are using outdated operating systems (such as XP) that are no longer supported by Microsoft and hence no patch exists.
NHS England have released an updated statement. Dr Anne Rainsberry, the NHS incident director, said:
We’d like to reassure patients that if they need the NHS and it’s an emergency that they should visit A&E or access emergency services in the same way as they normally would and staff will ensure they get the care they need.
More widely, we ask people to use the NHS wisely while we deal with this major incident, which is still ongoing. NHS Digital are investigating the incident and across the NHS we have tried and tested contingency plans to ensure we are able to keep the NHS open for business.
Here’s a little background from my colleagues Damien Gayle, Alexandra Topping and Sarah Marsh. They report the situation as it stood at about 5pm today:
Hospitals across England have been hit by a large-scale cyber-attack, the NHS has confirmed, which has locked staff out of their computers and forced many trusts to divert emergency patients.
The IT systems of NHS sites across the country appear to have been simultaneously hit, with a pop-up message demanding a ransom in exchange for access to the PCs. NHS England has declared a major incident. NHS Digital said it was aware of the problem and would release more details soon.
The NHS has declared a major incident after it was hit by a cyber attack that is thought to have affected services across England and Scotland. Staff have been locked out of their computers and many trusts have been forced to divert emergency patients.
We’ll be updating you here as this story develops.
The IT systems of NHS sites across England have been hit by a large-scale cyber-attack with a pop-up message demanding a ransom in exchange for access to the PCs. Hospitals across the country have staff who have been locked out of their computers and many trusts have been forced to divert emergency patients, the NHS has confirmed.
Details of patient records and appointment schedules, as well as internal phone lines and emails, have all been rendered inaccessible.
Share your experiences
Have you been affected by the cyber-attack? Perhaps you are in A&E awaiting to be treated, or are due to have an appointment with your GP. Whether you are a patient or NHS staff, you can share your experiences by filling in the form below, anonymously if you wish. We’d also like to hear from those working in the NHS.
We’ll feature some of your responses in our reporting.
Your responses are secure as the form is encrypted and only the Guardian has access to your contributions.
An Ebola outbreak has been declared in north-east Democratic Republic of the Congo, the World Health Organization (WHO) has said, after the virus caused three deaths since 22 April.
WHO said the outbreak had affected an equatorial forest region in Bas-Uele province, bordering Central African Republic.
The last Ebola outbreak in Congo in 2014 was quickly contained and killed 49 people, according to official figures.
In a television address, the country’s health minister, Oly Ilunga, confirmed the outbreak and urged the population not to panic.
“[The DRC] has taken all necessary measures to responde quickly and efficiently to this new outbreak,” he said.
WHO said it was working closely with Congolese authorities to help deploy health workers and protective equipment in the remote area to “rapidly control the outbreak”.
In 2013, an Ebola epidemic began in west Africa that killed 11,300 people in Guinea, Sierra Leone and Liberia and has left thousands more survivors with long-term health problems.
WHO was criticised at the time for responding too slowly and failing to grasp the gravity of the outbreak. An experimental vaccine was recently developed that WHO said could be used in emergencies.
A number of hospitals have been hit by a large scale cyber attack, NHS England has confirmed.
Hospitals across the country appear to have been simultaneously hit by a bug in their IT systems, leading to many diverting emergency patients. NHS England said it was aware of the problem and would release more details soon.
Meanwhile doctors have been posting on Twitter about what has been happening to their systems.
A screen grab of a instant message conversation circulated by one doctor says: “So our hospital is down … We got a message saying your computers are now under their control and pay a certain amount of money. And now everything is gone.”
If.ra (@asystoly)
Why would you cyber attack a hospital and hold it for ransom? The state of the world
There have have been several observations in the press and on social media in the past few years that some of the mannequins used to sell women’s fashion represent unrealistic and unhealthy body sizes. But until we started to look into it, the issue had not been researched properly, and the evidence was mostly anecdotal.
Back in 1992, researchers surveyed a handful of mannequins from the 1930s-1960s housed in museums. They concluded that real women of a similar body size would be so thin that they would be unable to menstruate. More than 80 years on, and with women in a very different societal position than previously, you might expect things to have changed.
Sadly, however, that’s not the case. Our newly published research concludes that the body sizes of mannequins being used to sell female fashion on the British high street today represent those of severely underweight women.
Unhealthily thin
In 2015, we conducted a formal study of mannequins by surveying all national chain fashion stores on the high streets of two cities in England – Liverpool and Coventry – that were using mannequins. In total, we visited 17 stores and got acquainted with 58 mannequins, 32 of which were “female” and 26 “male”.
What we found was that all of the female mannequins in these shops had body sizes that corresponded to that of an underweight human. We didn’t find a single female mannequin that was a normal body size on display.
Samantha Jenkins (@samanthajenkins)
Is it even humanly possible to be as skinny as this Topshop mannequin? pic.twitter.com/fDJSO88v2L
October 30, 2014
The “ultra-thin ideal” is something that I, and many others across the world, loathe. Size zero culture and glamorisation of unrealistic and unobtainable body sizes has meant that the “ideal” body size frequently and implicitly communicated to women is dangerously unhealthy.
Promotion of the ultra-thin ideal has been shown to cause women to be dissatisfied with their body size. And, in turn, this dissatisfaction is thought to be one step along the path of developing an unhealthy desire or “drive” for thinness, and subsequent eating disorders.
Not everyone will develop an eating disorder from having the ultra-thin ideal pushed upon them, and it is difficult to say why some people develop them and others don’t. However, the academic community is pretty convinced that promotion of ultra-thinness is a major player in eating problems, and that it is responsible for the propagation of body image problems in young women.
An ideal model?
Interestingly, we found that most of the male mannequins in our survey didn’t look underweight – only 8% of those surveyed were too thin. This fits well with what we know about ultra-thin body ideals and gender: it is primarily communicated to women, who are a lot more likely than men to develop an eating disorder like anorexia.
Mean mannequin sizes rated using the BMI-based body size guide rating scale. Photograph: Eric Robinson
Our observation of male mannequin shows that there is no legitimate reason why mannequins used to sell female fashion have to be ultra-thin. If their male counterparts can be a “human” shape and size, then why can’t they?
Although some nation fashion stores say they are using larger bodied mannequins, we found no evidence of this in any of the stores that we visited. Of course, we can’t rule out that there may be some larger mannequins knocking about in a small number of stores, but we found that unhealthily thin mannequins are the norm on the high street.
Mannequins aren’t people, nor do they have a sign on them saying “you need to look like this”. But they are representations of the human body that are used to sell fashion and the idea of beauty. There is clear evidence showing that the ultra-thin ideal is contributing to the development of mental health problems and eating disorders.
There is no excuse for the continued use of emaciated mannequins.
Eric Robinson is a senior lecturer in the department of psychological sciences at the University of Liverpool.
This article was originally published on The Conversation. Read the original article.
From nigiri to temaki, sushi has boomed in popularity in the west, but now doctors are warning of a less appetising trend: a rise in parasitic infections.
A team of doctors from Portugal raised concerns after a 32-year old man was admitted to hospital complaining of pain in his abdomen just below his ribs, vomiting and had a slight fever, all of which had lasted for a week.
An endoscopy soon revealed the culprit: the larvae of a type of parasitic worm from the genus Anisakis. The doctors note that the condition, known as anisakiasis, is caused by eating undercooked or raw fish or seafood that has been contaminated: indeed, questioning of the patient revealed that he had recently eaten sushi.
After the larva was removed the man rapidly recovered, say the medics.
Two views of the parasite, seen here firmly attached to an area of the patient’s upper gastrointestinal tract. Photograph: Carmo et al/BMJ case reports
Writing in the journal BMJ Case reports, the team warn that with sushi in vogue in the west, awareness of anisakiasis is growing.
“Most of the cases were described in Japan due to food habits; however, it has been increasingly recognised in western countries,” the authors write, pointing to a Spanish study that reported 25 cases of the condition over a three year period from 1999 to 2002, with all patients having eating raw anchovies, as well as Italian research which flagged both anchovies and sushi as routes by which individuals could become infected.
The Italian study added that medical professionals should suspect the condition should patients complain of severe abdominal pain after eating raw fish, pointing out that “no effective pharmacological treatment is able to kill the larvae once eaten”.
Indeed, as the US Center for Disease Control and Prevention notes, “The treatment for anisakiasis may require removal of the worm from the body by endoscopy or surgery.”
The authors of the latest report add that besides the symptoms shown in the Portuguese case, the condition can also trigger a host of other symptoms including severe allergic reaction, as well as complications such as digestive bleeding, bowel obstruction and peritonitis.
The Food Standards Agency noted that raw fish occasionally contain parasitic larvae, but said that under European food hygiene legislation fish that is to be eaten raw should be frozen before it is sold to consumers to ensure any parasites have been killed.
The FSA added that fish and meat should always be cooked properly according to the producer’s instructions, but offered a few tips to those planning to make their own sushi.
“If you do choose to make your own sushi from fish at home, ensure you follow a reputable recipe,” the FSA advised. “If wild fish are to be eaten raw or lightly cooked, ensure that all parts, especially the thickest part, have been frozen for at least four days in a domestic freezer at -15C or colder. This will ensure that any undetected Anisakis larvae are killed.”
I almost didn’t write this. It wasn’t from not wanting to. I cradled my head in my hands, desperate to contribute to the reams of social media positivity I had seen surrounding Mental Health Awareness Week.
I almost didn’t – couldn’t – because I was depressed.
There came a certain point in my experience of being LGBT where I accepted that I had to be strong and uncompromising in the face of disapproving glances and withering remarks. I made a pact to throw myself into my community with zeal, no matter how exhausting, and to make full use of the privileges I was afforded in the tolerant metropolis I’d landed in.
And yet, for some reason, I find this an incredibly difficult attitude to transfer over to my struggle with depression. I will share with my co-workers that I am going on a date with a man or going to an LGBT-themed event with an almost belligerent pride, but am overwhelmed with fear in having to admit to those same people that I’m leaving slightly early to see my therapist or that I need to take some time off due to another episode.
Indeed, the word “depression” still has a bite to it, in the way that the word “gay” did when I first dared to say it to someone else in reference to myself. The tone of my voice takes on an odd quality as I approach it in a sentence, to the point where I sound intolerably meek by the time “depression” tumbles out.
The thing is, in many cases, mental illness and being queer go hand in hand. It’s an uncomfortable but important reality that LGBT youth are four times more likely to kill themselves than their heterosexual counterparts. More than half of individuals who identify as transgender experience depression or anxiety. Even among Stonewall’s own staff, people who dedicate themselves to the betterment and improved health of our community, 86% have experienced mental health issues first-hand. It’s a morbid point to make, but it makes perfect sense that we, as a community, struggle disproportionately.
At a recent event I attended, set up to train LGBT role models to visit schools and teach children about homophobia, no one explicitly mentioned their struggles with mental illness. We told one another stories of how we had come to accept ourselves in the face of adversity, talking in riddles about “dark times” or “feeling down” or being a “bit too much of a party animal”. But these problems have other names – depression, anxiety, addiction – that we consistently avoid, despite being in a community in which a large percentage of us will have undergone similar experiences.
And this phenomenon replays itself over and over. Despite there being a common understanding between me and my queer friends that we’ve probably all been vilified in the same way and made to feel a similar flavour of inadequate, we will rarely acknowledge, even within the safe boundaries of friendship, that this has had a lasting impact on our ability to maintain a healthy self-image.
But part of being proud of who we are as LGBT people is being able to be open about the struggles we’ve faced. It’s in naming and wearing the uncomfortable badges of anxiety, depression and addiction that we take the first step towards fully accepting mental illness as an important part of our collective identity. After all, how can we be true role models to the next generation if we refuse to tell the whole story?
And so, this Mental Health Awareness Week, I’m issuing a challenge to my community. If you are LGBT and suffer from a mental illness, be defiant in your acceptance of it in the same way that you would about your sexuality or gender identity. Bring it up, speak it out and feel sure that your voice, however seemingly small or insignificant, is a valid one. After all, we have been, and will always be, a community of fighters – it’s about time we dared to show our battle scars.
Brazil has declared an end to its public health emergency over the Zika virus, 18 months after a surge in cases drew headlines around the world.
The mosquito-borne virus was not considered a major health threat until the 2015 outbreak revealed that Zika can lead to severe birth defects. One of those defects, microcephaly, causes babies to be born with skulls much smaller than expected.
Photos of babies with the defect spread panic around the globe as the virus was reported in dozens of countries. Many would-be travellers cancelled their trips to Zika-infected places. The concern spread even more widely when health officials said it could also be transmitted through sexual contact with an infected person.
The health scare came just as Brazil, the epicentre of the outbreak, was preparing to host the 2016 Olympics, fuelling concerns the Games could help spread the virus. One athlete, a Spanish wind surfer, said she got Zika while training in Brazil ahead of the Games.
In response to the outbreak, Brazil launched a mosquito-eradication campaign. The health ministry said those efforts have helped to dramatically reduce cases of Zika. Between January and mid-April, 95% fewer cases were recorded than during the same period last year. The incidence of microcephaly has fallen as well.
The World Health Organization (WHO) lifted its own international emergency in November, even while saying the virus remained a threat.
“The end of the emergency doesn’t mean the end of surveillance or assistance” to affected families, said Adeilson Cavalcante, the secretary for health surveillance at Brazil’s health ministry. “The health ministry and other organisations involved in this area will maintain a policy of fighting Zika, dengue and chikungunya.”
All three diseases are carried by the Aedes aegypti mosquito.
But the WHO has warned that Zika is “here to stay,” even when cases of it fall off, and that fighting the disease will be an ongoing battle.
Like church and state, medicine and politics are traditionally seen as a queasy mix. The last thing you want in your flimsy hospital gown is some zealot with a stethoscope trying to sway your vote. Doctors, at the bedside, should clearly stick to doctoring. But – in a world of ever more outlandishly spun health statistics – where, outside of clinical encounters, do the limits of doctors’ duty to act in our patients’ best interests lie?
I made the sobering discovery, in my first few weeks as a doctor, that serving patients in the modern NHS was at least as much to do with advocacy as medicine. It has to be, in a system that’s stretched beyond breaking point. With resources so scarce, speaking out counts.
Once, I actually stalked a professor, in sheer desperation to provide an inpatient with decent care. He did a double take at the steely-eyed junior doctor, sat perched outside his clinic, fired up to plead her patient’s case. With everyone run ragged, overwhelmed by patients, no one had believed me or cared enough to act when I’d insisted my patient was suffering from a rare diagnosis, adult-onset Stills disease, that had left her heart swamped in fluid, her temperature soaring, her circulation so fragile it might need intensive care. “Please,” I begged. “Just see her for yourself.” As the pre-eminent professor of rheumatology in my hospital, he was the one man I knew who might act. And he did. He confirmed the diagnosis and whisked my patient off to his specialist care, possibly saving her life.
When almost every statistic about today’s NHS depicts a system quietly imploding around us, advocacy writ large has never mattered more. Doctors, like nurses, bear daily witness to the facts behind the spin. Our testimony is a vital corrective to a government hell-bent on airbrushing away the truth about today’s underfunded NHS. We look the patients in the eye as they languish on trolleys in hospital corridors. We apologise, shamefaced, to the families whose loved ones are stranded in hospital, because no social care exists to support their safe discharge home. We turn away the elderly who sob in A&E because the pain in their hip is beyond endurance, yet who haven’t even made it on to a waiting list for surgery. If we turned a blind eye and kept our heads down, would Hippocrates nod his assent?
Having to break bad news to a patient is never easy. But unflinching conversations are a cornerstone of good medicine
The state of the NHS in 2017 demands that doctors speak out about the human cost of underfunding since it clear our political leaders will not. Only this week, Theresa May made an election manifesto commitment of 10,000 more staff in mental health. Unfunded, needless to say, but also – more audaciously – a promise made on the back of the 6,700 mental health staff already culled since the Conservatives came to power in 2010. It’s this kind of political doublespeak that compels doctors to challenge loudly the government line that – despite the most brutal funding squeeze in NHS history – everything is going swimmingly.
In microcosm, we already know what happens when cost-cutting is prioritised above patient care. The scandal of Mid Staffs – a stain upon the history of the NHS, in which patients in their thousands were subjected to inhumane care – arose when one hospital trust strove to slash costs by millions. Yet currently, the government is enforcing £22bn of “efficiency savings” across the NHS, while insisting excellence of care can somehow continue.
Doctors should call out this claptrap for what it is. We are, after all – perhaps more than anyone – trusted to tell unpalatable truths. In this case, the hard medicine is more taxes. A world-class health service requires world-class funding. Either we provide the budget to fit the health care we want, or we cut the NHS to fit the amount we’re willing to spend on health. With a government too cowardly to confront this simple truth out loud, doctors should force an honest debate.
Yet – with a few notable exceptions (Taj Hassan and Neena Modi, for example, the presidents of the Royal Colleges of Emergency Medicine and of Paediatrics and Child Health respectively), the medical establishment is loath to rock the boat. Where is the joint statement from the Royal Colleges, for instance, urging increased taxation to bring our NHS and social care spend to at least the levels of Germany and France? Where are the hospital medical directors brave enough to speak out in public against the ever more fanciful diktats from on high to keep on delivering as their funding dries up?
Having to break bad news to a patient is never easy. But unflinching conversations are a cornerstone of good medicine. Nationally, doctors should be telling it like it is: without more money, our NHS is in relentless, terminal, and wholly avoidable decline.