In proportion to their collective contribution to human suffering, neglected tropical diseases (NTDs) have received insufficient attention. Today, thanks to incremental progress in the science of public health, growing programmatic experience and commitment from endemic country governments, donors and other partners, we are better equipped than ever before to recognise, prevent, control, eliminate and eradicate them.
Trachoma is one of many NTDs that are rooted in poverty. It is an infectious disease of the eye caused by a bacterium, and marked in its early stages by inflammation of the inner surface of the eyelid. Infection is spread by the transfer of discharges from the eyes or nose of an infected person.
More severe manifestations, such as trichiasis, typically occur in adulthood after multiple untreated infections. Trichiasis is present when turned-in eyelashes scratch the eyeball – a debilitatingly painful condition that may lead to progressive and irreversible visual impairment.
At present, about 0.45 million people are blind and 1.4 million people are severely visually impaired as a result of trachoma. Very basic interventions – simple eyelid surgery, the antibiotic azithromycin to clear infection and facial cleanliness, water and sanitation – can significantly reduce the impact of the disease. These interventions (surgery, antibiotics, facial cleanliness, environmental improvement) are represented by the acronym Safe: the strategy recommended by the World Health Organisation (WHO) to eliminate trachoma as a public health problem globally by 2020.
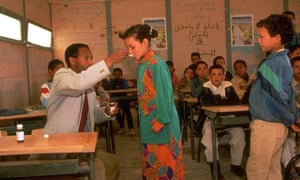
Morocco succeeds with Safe
Morocco adopted Safe in the early 1990s, becoming the first country to implement the strategy at national scale and one of the first to benefit from Pfizer’s now long-running donation of azithromycin to trachoma elimination programmes.
In November 2016, Morocco was validated by the WHO as having eliminated trachoma as a public health problem, joining Oman and Mexico as the only countries documented to date as having beaten the disease. Other countries have made similar progress, and further official validations are likely to follow later in 2017.
Mapping trachoma
Trachoma’s natural home is among populations who live furthest from services, and so, until recently, data on where to intervene were grossly incomplete. The Global Trachoma Mapping Project (GTMP) sought to remedy this with surveys covering more than 1,500 districts in 29 countries. The project was completed in just over three years – running from December 2012 to January 2016 – and involved the training and deployment of more than 600 field teams, who collectively examined more than 2.6 million people. Its successful implementation now provides health ministries with the information they need to plan interventions, where required, for worldwide trachoma elimination.
Visionary backing
The success of the mapping project is attributable to a number of factors. First, it had financial backing from the UK’s Department for International Development and the United States Agency for International Development. Second, in each of the countries in which the GTMP operated, it benefited from high-level political commitment and strong health ministry leadership. Third, a worldwide partnership of NGOs and academic institutions, spearheaded by Sightsavers, the International Trachoma Initiative and the London School of Hygiene and Tropical Medicine, fostered synergies rather than inter-organisational competition. Fourth, the mapping project was held to strict quality standards, despite operating in some of the most difficult environments in the world. And fifth, the mapping was innovative in its use of technology, which kindled the interest of partners on all sides.

Field teams collected all data into a purpose-built app running on Android smartphones. Those data, including geospatial information, were uploaded to a secure cloud-based server as soon as the phones were within range of a suitable network. Raw data were then cleaned, reviewed by the health ministry, and once approved, automatically displayed on the online Trachoma Atlas. This system was far more rapid and reliable than previous paper-based survey tools – and saved approximately 4.2m sheets of paper.
Work is ramping up in the 42 countries where trachoma remains a public health problem. In the next few years, with continued political support, collaboration and donor investment, we will finally be able to write the closing chapters in the long history of this devastating disease.
Victor Florea is an intern and Anthony Solomon is a medical officer for trachoma in the Department of Control of Neglected Tropical Diseases, World Health Organisation.
Join our community of development professionals and humanitarians. Follow @GuardianGDP on Twitter.
Neglected no more: ending trachoma, an infectious eye disease rooted in poverty