The Indian government’s new maternity bill, which comes into force this week, has been branded an elitist policy that will do little or nothing to help the vast majority of the country’s mothers.
According to women’s groups, the new rules – which raise maternity leave from 12 to 26 weeks, putting India ahead of France and the US – will apply only to a small fraction of the female workforce.
“It’s as if, for the government, 95% of India’s women don’t even exist,” said Juin Dutta, from Paatshala, a group helping impoverished female handicraft workers. She pointed out that the extension will only apply to women in the formal sector, which amounts to just 5% of India’s working women.
India’s prime minister, Narendra Modi, hailed the bill as “a step forward for Indian women” when he introduced details of the legislation on his monthly radio address this week.
“The basic aim is to ensure proper care of the newborn, the future citizen of India, from the time of birth,” he said. “The newborn should get the complete love and attention of the mother. That is how these children will become true assets of the country when they grow up. Mothers too will remain healthy.”
Internationally, the bill has been touted as a success for India, which has one of the world’s lowest female employment rates – 25% – and where mothers often feel under pressure to leave their jobs after having children. A headline in Fortune magazine said India’s move “puts the US to absolute shame”.
But most Indian women will never reap the benefits, according to the International Labour Organisation. “India’s informal economy is huge, it employs over 435 million men and women who never see the benefits of government laws,” said Aya Matsuura of the ILO.
“In the informal sector, you never have to sign a formal employment contract and your relationship with the employer is unclear. For example if women work as maids – and up to 10 million Indian women work as domestic cleaners or cooks – they will not have signed a contract. They have a verbal agreement, so in reality they are not really covered by formal rules and are not recognised by law.”
Those working in the informal industries are among the most vulnerable, Matsuura said: “They have problems. If a woman gets pregnant, she has to find a temporary replacement for herself, like a sister or a sister-in-law. Otherwise, she loses the job.”
Pratibha R, of the Garment and Textile Workers Union in Bangalore, said the bill did little to resolve the problems of working mothers. “Our members are entitled to the 26 weeks, but what happens after? According to the new law, workplaces are supposed to provide creches on site, and women are supposed to be able to go see their babies four times a day, but in practice that doesn’t happen.
“The facilities provided are unclean and low quality, women don’t feel comfortable leaving their babies there. Women are very afraid to leave small babies there, and so they just leave after pregnancy.”
A pregnant female worker at a construction site in Ahmedabad, in India’s Gujarat state. Photograph: Dinodia Photos/Alamy Stock Photo
A survey by the Associated Chambers of Commerce and Industry suggests that a quarter of women in India don’t return to work after having their babies.
Reducing that number could increase India’s national income by 27%, according to the International Monetary Fund.
But increasing female participation in India is complex, said economist Rupa Subramanya. Maternity benefits may make women more willing to work, but they also make employers less willing to hire them.
“India is still a developing country. Countries like Norway can afford to give mothers a year’s maternity leave now but they didn’t have that while they were still developing,” Subramanya said.
LocalCircles, a citizen engagement organisation that surveyed more than 4,000 small businesses about the new maternity rules, found that 26% of firms said they would favour men over women because of the new rules.
Yatish Rajawat, chief strategy officer for LocalCircles, said: “There is a lot of political correctness on hiring for diversity. Many people say something and do the opposite. The fact is that business dynamics will take over politically ‘right’ things. Now businesses are looking at women and thinking I’ll have to pay two persons’ salary for one person’s work. Now employers will not just look at women’s qualifications and capability but also the fact that they come with an additional cost.”
One solution, according to Naiyya Saggi, founder of BabyChakra, India’s largest online community of mothers, would be to introduce paid paternity leave. “When an employer is deciding between a man and a woman, the burden of parental leave should be equally shared,” said Saggi. “The government hasn’t put in place proper childcare infrastructure for women, and instead has passed that burden on to employers.”
She said women still feel taking any time off would have a negative impact on their careers. “Six months is a long time in today’s world, with automation and artificial intelligence. Mothers already feel they need to be reskilled after taking that much time off.”
But Nidhi Gupta from the Takshashila Institute, a thinktank, said the law was a step in the right direction despite its limitations.
She said: “Women bring as much skill and talent to the table as men do. We go to the best schools, best colleges, as we are as talented and skilled as men are. So why should we be excluded?”
The argument that employers will be reluctant to hire women over maternity leave is unproven. “In the UK, when they introduced the Equal Pay Act, the same argument was made,” said Gupta. “But actually studies have shown that it has not made employers less willing to hire women.”
Thousands of disabled people face long delays to receive an NHS wheelchair, the first official figures on the subject show.
One in five children who need a wheelchair are being forced to wait beyond the supposed maximum 18 weeks, as are almost one in six adults. Campaigners say the figures reveal a “postcode lottery” in provision across England.
Some 7,200 people who received a wheelchair between October and December had waited at least 19 weeks, despite the NHS Constitution guaranteeing access to one within 18 weeks.
NHS England does not record how long over the 18-week threshold patients have waited for a wheelchair. But the charity Muscular Dystrophy UK says it knows of young adults who within the past year had waited more than eight months.
The NHS England figures obtained by the Health Service Journal (HSJ) show that those with the greatest need for the equipment can face the longest waits.
Nic Bungay, director of campaigns at Muscular Dystrophy UK, told HSJ that long waits for a wheelchair appropriate for their needs were stopping young people “going out independently … and accessing university, work and friends”.
An estimated one in 50 Britons is believed to use a wheelchair to go to work or school, get to the shops, look after their children or undertake other tasks. The Wheelchair Alliance, led by Paralympic champion Lady Grey-Thompson, claims “great variation in ability to access assessment and obtain service provision”, as well as delays in receiving equipment and having it repaired, were affecting too many people.
The campaign group is urging the NHS to ensure equality of access for everyone who needs a wheelchair, which “would prevent confusion and disadvantage when education needs mean a user moving to another area or changing their GP [and put] an end arbitrary age discrimination. This is especially the case where very young children may or may not be provided with chairs depending solely on where they live.”
Almost 40% of adults with high or specialist wheelchair needs, who are defined as “fully dependent on their wheelchair for all mobility needs”, wait more than nine weeks for the NHS to decide what kind of wheelchair they need. A further 37% wait more then nine weeks to then receive their equipment. Slightly smaller numbers of children with the same level of need have to wait the same lengths of time, the HSJ discovered.
The data also shows that waits for wheelchairs lengthened significantly between April and June and the last three months of 2016, especially for adults.
NHS England said it accepted that some local NHS clinical commissioning groups needed to get wheelchairs to those in need more quickly.
“While the majority of children and adults get their wheelchairs within a few weeks, there are parts of the country where local services are not sufficiently responsive and we fully agree that needs to change,” a spokesman said.
The organisation has pledged to halve the number of children waiting more than 18 weeks by April 2018 and eliminate overly long waits for anybody by April 2019.
During a recent 10-day stay in a London hospital I impertinently asked each of the 49 people who came to my bedside where they were from originally. Ten were British, five Portuguese, four Spanish, three Philippino, two each from India, Ghana, Somalia and Finland, and one each from France, Germany, Italy, Poland, Ireland, Romania, South Africa, Sierra Leone, Nepal, Brazil, Ethiopia, Malawi, Zaire, Malaysia, Mauritius, Eritrea, Sri Lanka, Iran and Nigeria. These figures should mean something to politicians. They certainly meant a great deal to me and to my fellow ward-mates. John Holme London
• On page 29, Balancing the Bookshelves calls for better gender balance in children’s books (18 March), including not assuming animal characters to be male. Page 33: Natalie Nougayrède writes of “the inalienable dignity of mankind”. Page 38: “cameraman” (but on page 47 “camera operator”). Would it be too much to ask this paper to practise what it preaches? Sylvia Rose Totnes, Devon
• Can these 7 million wasted takeaway coffee cups per day not be sent to plant nurseries for potting (Cook, 11 March)? Rupert Stringer Horley, Surrey
• Now that we know when the PM will trigger article 50 (Report, 20 March, theguardian.com), will Wednesday 29 March 2017 go down in remainers’ diaries as May Day (Mayday, Mayday)? Colin Barr Ulverston, Cumbria
• In Hyde, in the 1950s, my mother would sandwich two rounds of leftover pastry with jam, brush the top with milk and bake (Letters, passim). This went by the name of courting cake. My three sons, irreverent southerners, renamed it leg-over cake. Jane McAdoo London
• In the Centerprise community project (Hackney, early 1970s) we used to sell, successfully, caterers coleslaw enhanced with raisins and fresh apple as “social workers’ salad”. Tom Wilson Nottingham
• Join the debate – email guardian.letters@theguardian.com
• Read more Guardian letters – click here to visit gu.com/letters
A study suggests that average life expectancy will soon exceed 90 for the first time. Women born in South Korea in 2030 are forecast to have a life expectancy of 90, with other developed countries not far behind.
France is second in the league table for women, at 88.6 years, with British women 21st, at 85.2 years, and British men 14th, at 82.5 years.
We asked men and women in their 90s what life has taught them about ageing. Here is a selection of our interviews.
Jean Miller, 94, from Falkirk: ‘Life is an education. I’ve realised there’s a rhyme and reason for everything’
The key to reaching such a good age is to keep active and interested in things. I was working in a salon up until last year, but I had to leave as I was feeling a few aches and pains. I didn’t want it to get to the point where management asked me to leave. I used to take coats and make sure all the guests through the door were attended to. I made lots of great friends this way.
The moment you stop and sit in a chair is when you struggle. I have a lovely family and have taken an interest in the world around me. Now I am no longer working I go to a gym class on a Monday. It’s a class for over 50s so it’s fun, enjoyable exercises. We have tea afterwards. I also joined the University of the Third Age, a group for retired or semi-retired people to get together and learn for fun. There’s a theatre group I am part of through this and I am also hoping we will get to learn German soon. I signed up but we need a few more people to get involved before we can get started.
Life is an education and if you don’t learn as go along then that’s bad. I’ve learned to see things in a different way over time. My biggest lesson is to be more patient. I used to worry about things but now I don’t. I’ve realised there’s a rhyme and reason for everything. In life you’ve got to take things as they come.
Pam Zeldin, 94, from Manchester: ‘Get enough sleep, and don’t drink to excess – that said my older sister does enjoy a little G&T’
Pam Zeldin, 94 (left) with sister Nora, 98, and granddaughter Sophie. Photograph: Sophie Zeldin-O’Neill
I live with my sister Nora, who is 98, and we look after each other. Ten years ago her husband died and both her daughters were living in France at the time, so I said she could come and stay with me. We have always got on very well, and work as a team. We do all our own housework and have a chap who comes to tend to the garden. We clean the house together – she does the upstairs and I do downstairs. She cooks, and I do everything I can to help.
My main advice for people who want to live to a good age is to look after your health and live moderately. Also, get enough sleep, and don’t drink to excess – that said, Nora does enjoy a little G&T in the evenings!
When I retired, I joined a local choir and the Townswomen’s Guild. Getting involved in the community is really important as you get older because it broadens your social circle and your interests. I have always tried to get out a lot. I have two daughters, one of whom lives very nearby, so she often gives us a lift, or we’ll get a taxi. She also takes us on trips to places nearby, which we really enjoy. I have a scooter which comes in very handy and we have a little push trolley for when we go shopping. We also go to the cinema and the theatre, and on coach trips around the country. We go to the library and get our medicines delivered. We can’t go too far but we manage just fine.
I have learned that tolerance and routine is good. And to look after yourself and stay as active as possible. Being in your 90s is not as fun as other ages because you’re not as active, and your mobility is restricted. But you have to learn to cope as best you can. We have visitors – my other granddaughter who lives in London has come to Manchester University, so I am here for her at any time. It’s wonderful having grandchildren in the family.
What would I tell my younger self? I think I’ve done ok, but I would say, start as early as you can to make yourself financially stable for when you get older, so that you don’t have to worry. Take advantage of every opportunity – don’t just sit in the house. Also, travel as much as you possibly can – see the world, live well, take care of yourself. But don’t take things too seriously – it’s important to have lots of fun along the way too.
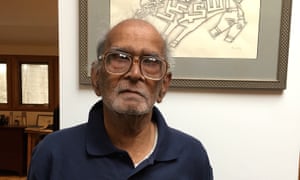
Krishnamoorty Dasu, 90, New Jersey, US: ‘To a great extent, age is just a state of the mind’
Krishnamoorty Dasu, 90: ‘The most important thing: be useful to yourself and to others.’ Photograph: Tamraparni Dasu
I’ve made it to this good age simply because death has been kind enough not to knock on my door.
I enjoy my life, it is a gift. Negotiating it itself is fun. Old age is what others attribute to you. To a great extent, age is a state of the mind. I take pleasure from listening to music and reading fiction. This is what I do for enjoyment these days.
I have learned a lot over the years but the most important thing: be useful to yourself and to others. If I could send a message to my younger self it would be to keep your mind and body fit by reading and rumination and through walking exercises. Also, eat in moderation. You really do not need all that food you eat.
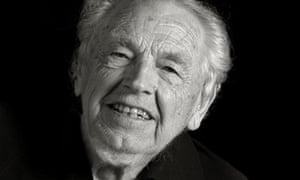
Don Anderson, 99, from Birmingham: ‘You’ve got to take life and love gently, avoid the stresses’
Don Anderson, 99: ‘After my wife died, I tried internet dating. But it didn’t work out’
My advice for living to a good age is to take life slowly. This means avoiding the stresses that go with a lot of jobs. Find something peaceful to do like I did. My career was varied. I ended up actually founding Harlow, a local government district in the west of Essex. I bought the land it was built on and set up a council. I was one of the area’s founding fathers. I was a land agent before that and later in life became a professor.
I don’t have a great deal of hobbies now but I read a lot and I also keep active online. I use my iPad a lot. I’ve learned a lot over the years, but as I said above the biggest lesson is to take life in a measured and relaxed way, not to rush or worry too much about things. The same goes for what I have learned about love. My wife died some time ago and I tried internet dating after that. But it didn’t work out. You’ve got take love gently too.
Sheila Keating, 91, from London: ‘I have actually gained interests. I never used to write but I do that quite a lot now’
Sheila Keating, 91: ‘ I don’t eat particularly healthily. I don’t exercise enough’
Life in your 90s is much slower because I have difficulty with movement. But luckily I am not slower intellectually. I have actually gained interests. I never used to write but I do that quite a lot now. In fact I have written my husband [HRF Keating’s] biography and am waiting to get it published. I also record audiobooks.
One thing I hate though is modern technology. I use it of course but bitterly resent how much it’s used. There’s no other option in many cases. I think this is wrong because it doesn’t always work.
What have I learnt over the years? I am more tolerant than I used to be. That doesn’t mean I don’t champion certain causes I am passionate about but I live with others’ way of life more readily. That’s a plus for when you get older.
My biggest pleasures include having supper with friends and family. I go to the theatre still, not so much west end as it’s too expensive. I used to go swimming but have had to cut back on physical activities now. That’s one of the negatives of getting to this age.
I think I’ve managed to live this long due to sheer luck. I don’t eat particularly healthily. I don’t exercise enough although I used to more. I don’t think you can say any one thing is the key to a long life. All I know is that you’re extremely lucky if you keep your health into your 80s. You are there and ploughing on until 100 – that’s where I aim to get to.
One morning at breakfast our daughter, Laila, looked up from her cornflakes and said: “Why am I the only child in this family?”
We had always known we wanted more than one child. Laila was born in 2011, a year after Bridget and I married. I loved being a dad. Children are hope in human form and while parenthood was often challenging, it also gifted us an addictive joy.
Soon after Laila turned one, Bridget suggested we try for a second baby. We wanted another child because, to us, having only one made us feel as if our family were incomplete. We wanted Laila to have a sibling and felt we would be failing her if we did not give her the chance of being someone’s big sister.
Bridget got pregnant easily the first time, so we assumed she would do so again. To begin with, we did not pay much attention to the monthly disappointments. But, in time, I came to dread the sound of heavy footsteps as Bridget returned from the bathroom having spotted the blood that indicated her period was coming and a baby was not. She would curl back into bed with me and I would hear her quietly crying.
Sarfraz Manzoor with his daughter, Laila, when she was eight months old. Photograph: Graham Turner for the Guardian
We moved from trying and then struggling and then failing to fall pregnant. The more we tried, the less fun it became. Sex went from pleasure to duty, from spontaneous to scheduled. It did not matter if we had had a fierce row earlier in the evening – by the time we got to bed we would somehow need to kiss and make up. Meanwhile, friends’ pregnancies produced new siblings for Laila’s friends.
After more than a year of failure, we saw our doctor. No single factor appeared to explain why Bridget was not getting pregnant. It had never occurred to us that we might have fertility problems – we already had a baby – but having failed to conceive naturally, we were advised to consider IVF. The fact that we had Laila meant the NHS would not pay and that we would have to go private – at a cost of thousands of pounds. It would eat up my savings, and there was no guarantee of success, but we felt we had at least to try, so that Laila could have her longed-for younger sibling.
We agreed to start on IVF and a few days later two large cardboard boxes arrived at our home filled with drugs for Bridget. There were also fearsome-looking syringes for injecting drugs into her stomach. Meanwhile, I signed up for weekly acupuncture sessions that aimed to boost the mobility of my sperm, and started taking special sperm-enhancing vitamin tablets. The drugs worked: within a couple of months, Bridget had produced a cluster of eggs, two of which were then fertilised. On 26 June 2015, the two embryos were transferred into Bridget’s uterus.
We then had to wait two weeks for the all-important pregnancy test. We hardly slept the night before. That morning, with Laila still asleep in her bedroom, I pulled out a framed photograph of our wedding day. We stared at it. What we were going through was nothing compared with those having IVF who did not already have children. Whatever the result of the pregnancy test, we had a huge amount to be grateful for.
A blood test revealed that it was good news: Bridget was pregnant. We were elated: all that money and all the pills and needles had been worth it.
The following weekend, I headed off to the Latitude festival, while Bridget was booked in to have some blood tests. On the Sunday, I noticed a missed call from Bridget. She had heard from the clinic: her pregnancy hormones were not increasing as fast as was expected. It could be ominous or it could be nothing – the only way to know was to book in for a scan.
The scan revealed that there was a gestational sac – a first sign of early pregnancy – but in order to tell whether it was still growing, a follow-up scan was needed. At the second scan, the nurse said, “I can see the heart beating.”
Bridget burst into tears of happiness and we hugged each other as the nurse said we should book for a third scan to track the rate of the embryo’s growth. It felt like a formality. The scan was scheduled for 10 August, the day before Laila’s fourth birthday. It would, we thought, make a perfect pre-birthday present if she came with us and got a glimpse of her future sister or brother.
That summer morning, we walked into the room full of sunny confidence. I sat next to Laila holding her hand and Bridget lay on her back as the nurse examined her. She worked in silence, studying the cloudy images on the monitor. We had become used to the routine. The nurse completed her tests and then said, “I’m so sorry but it’s bad news: there is no heartbeat.”
I thought I had heard wrongly but Bridget understood. I was mute from shock – I could not believe what I had heard. Laila was wondering what had happened. “Are those happy tears, Mummy?” she asked.
When I recall the days after the news, what I most remember is Bridget and me weeping, sometimes together and at other times apart while trying to keep our distress from our daughter.
Bridget felt it was worth having one more attempt. She didn’t have the desire to keep going endlessly, failed round after failed round. It would be too hard on her body and mind, but she wanted to have one more try. The failed round of IVF had cost more than £12,000. We couldn’t afford a second cycle. It was then we had an unexpected stroke of good fortune: an uncle of Bridget’s generously offered to help to pay for a second round of IVF.
The whole business started again – the drugs and injections, the hope and the waiting.
One morning in mid-March the following year we did the pregnancy test and although the news was good, we could not allow ourselves to believe that success was inevitable. In the past, miscarriages had been something that happened to others, but they were now part of our story: we were too frightened to take anything for granted again.
I had a miscarriage. Why can’t we talk about losing a baby?
Even when blood tests confirmed the pregnancy and the scan revealed the tiny beating pulse of a heart, we could not allow ourselves to get too excited. Only when we went to the 12-week scan, which showed the embryo growing normally, did we feel safe enough to believe that our luck had changed.
It was a Saturday night and Bridget and I were at a friend’s wedding in the Devon countryside. She was 13 weeks pregnant and starting to show. The wedding disco had just begun and I was on the dancefloor. When I stepped outside the hall for some air, I saw Bridget. She had a stricken expression and I knew instantly that something had happened. “I’ve started bleeding,” she said.
Minutes later, she was sitting on the toilet in our hotel room, blood streaming between her legs. An ambulance crew advised us there was little point in being driven to A&E because they would not be able to confirm a miscarriage.
The next day we found ourselves in our local hospital as a sonographer smeared lubricating gel on Bridget’s belly. I am not sure we would have coped with a second miscarriage but, thankfully, the baby was fine – apparently the sort of bleeding Bridget had experienced was common but rarely discussed.
It was Sunday evening, 20 November, and Bridget was due to be induced the following day. She had been having minor contractions during the afternoon and by the evening they were becoming more intense. While we were having dinner, she said we should call for a taxi to take us to hospital. We reached the hospital at 9pm; an hour later, our son, whom we would later name Ezra Zakariya Manzoor, was born.
The following day, Bridget’s cousin brought Laila to the hospital. Bridget was in bed cradling our baby son when our daughter walked up to him. Bridget smiled broadly and said: “Laila – say hello to your little baby brother.”
The doctor will see you now. But for how long? This week the president of the Royal College of General Practitioners, Dr Helen Stokes-Lampard, said GP consultations in the UK are too short for people with complex health needs.
The average consultaton time in the UK is 10.6 minutes. This figure comes from a 2015 survey by the Commonwealth Fund on behalf of the Health Foundation, which surveyed 12,049 doctors in 11 countries. It was the second-lowest: only Germany had shorter consultation periods, at 10.3 minutes. But in Germany 80% of patients get less than 15 minutes with their GP, compared with 92% in the UK.
There is no standard time in the UK: it’s up to GPs to set the duration of appointments. But Stokes-Lampard told the BBC: “We’ve got a crazy situation whereby GPs are ridiculously overworked, there are too few of us and the whole situation is on the brink.”
Methodology: the survey of 12,049 GPs and primary care physicians in 11 countries, including 1,001 GPs in the UK, was carried out between 2 March and 8 June 2015.
Where you live in America predicts not just how long you’ll live but also how you’ll die. The “Black Lung mountains” run along the border of West Virginia and Kentucky. They are the epicenter of the so-called “hillbilly heroin” epidemic. In the lower Mississippi there’s “Cancer Alley” and heart attack valley. Violent deaths lead the list in the Far West, Alaska and Native American reservations. When it comes to health, one thing is clear: the US is not one nation. It is many.
In an analysis of 80 million deaths in the United States between 1980 and 2014, a study published on Tuesday finds dramatic differences not only in life expectancy, but also in cause of death from county to county. “We’re not narrowing the gap. The gap is widening,” said Christopher J L Murray, one of the authors of the study.
Their analysis shows that our health differs by geography as well as race, socioeconomic status and political culture. One particular hotspot has emerged: the border between Kentucky and West Virginia. The region is plagued by not only mental illness and substance abuse – which have received much attention in the media – but also chronic lung disease, cancer, cardiovascular disease, diabetes, motor vehicle accidents and common infections like diarrhea and pneumonia.
In Appalachia, many of the largest coal deposits have been exhausted. To access the smaller deposits, miners have to blast through a lot more rock, not just coal. All that blasting releases more dust and more toxic dust into the air. The result has been that between 2000 and 2012, there was a nine-fold increase in the most severe form of Black Lung.
As jobs have evaporated, diseases of poverty are exploding along the Kentucky-West Virginia border. Deaths from common infections have gone up in and along the Kentucky-West Virginia border as well as in the lower Mississippi Valley. Deaths from cardiovascular disease and diabetes are also up.
If environmental protections are further weakened and the Affordable Care Act is dismantled – and with it Medicaid expansion in Kentucky and West Virginia – the health of the region may well sink further.
The lower Mississippi is another death hotspot, most notably the Arkansas-Mississippi border and Louisiana’s “Cancer Alley,” but also extending towards Missouri, Oklahoma and Alabama. Like Appalachia, the Deep South is anti-union and anti-regulation; just swap coal mining for the oil, gas and petrochemical industries, and many of the same factors are at play. As in Appalachia, environmental contamination is driving higher rates of cancer and lung disease.
More than elsewhere in the country, social class in the Deep South is taken as evidence for what one deserves in life—also known as the just-world hypothesis—so it’s no surprise that support for social safety nets, including the Affordable Care Act and Medicaid, are weakest here. Arkansas is the only state in the Deep South to have expanded Medicaid. Along with the southwest and Alaska, the Deep South has the highest proportions of uninsured – this causes diseases of poverty to flourish.
While poor white and black Americans both have worse health in the Deep South than in most other parts of the country, black people also continue to suffer from racial discrimination and segregation. In earlier research, Murray showed that poor black Americans in the Deep South and in cities with high homicide rates have the highest mortality rates in the country.
Race creates a geography of its own – especially when you factor in residential segregation. According to David R Williams, a social science researcher at Harvard University “For many Americans, your zip code is a stronger predictor of how long and how well you will live than your genetic code.”
Research on the geography of health will help local health departments focus on the most urgent health problems and will arm citizens with the data they need to advocate for better health in their communities. But it’s important to remember that the geography of health is intertwined with the local political culture and local economy.
Not only do diseases vary county to county (and on an even more micro level), but solutions that may have worked to curb disease in one region—environmental and occupational regulations, for example—may not be palatable elsewhere without fundamental changes in the local culture and how people make a living.
In this age of inequality, none of the symptoms of our malaise can be ignored without consequence. It is up to us all to find out why some Americans are so much worse off than their compatriots – and close the gap fast.
Clove is one of the highly prized spices, native to the Maluku islands in Indonesia. The spice actually is dried aromatic flower buds of an evergreen rainforest tree in the family Myrtaceae, Sygizium aromaticum
It is available throughout the year and commercially harvested primarily in Indonesia, India, Pakistan, Sri Lanka, Madagascar, and Zanzibar. It is widely recognized all over the world for its medicinal properties and culinary qualities.
The spice is widely used in Asian, Middle-East, and African cuisines in the preparation of curries, gravy items, and marinades. It is used along with other spices, including cinnamon, cardamom, and black pepper in the cooking of Biryani (spiced rice).
Clove essential oil is used as an active ingredient in cosmetic products and the healing of many disorders. In the Middle East, it is added to beverages, at times along with cardamom and peppermint.
Clove has been used for thousands of years in India, China, and South East Asia, not only as a spice and condiment but also as a remedial herb for many ailments. Ayurvedic practitioners, for instance, use clove for tooth decay, halitosis, and bad breath, among others. In Traditional Chinese medicine, clove is considered an aphrodisiac.
Scientists have determined and isolated many bioactive compounds from clove, including (but not limited to) phenolic compounds: flavonoids, eugenol, hydroxybenzoic acids, hydroxycinnamic acids, and hydroxyphenyl propene; phenolic acids: gallic acids and its derivatives, hydrolyzable tannins; and other phenolic acids: caffeic, ferulic, ellagic and salicylic acids. Flavonoids found in lower concentration in cloves, including kaempferol, and quercetin and its derivates (glycosylated) .
Clove flower buds contain up to 18% of essential oils, which comprises, eugenol, eugenol acetate, humulene, geranyl acetate, and caryophyllene oxide. Other volatile compounds present in lower concentrations in clove essential oil are beta-pinene, farnesol, limonene, benzaldehyde, 2-heptanone and ethyl hexanoate.
Clove is considered as an important medicinal plant due to the wide range of pharmacological effects owed to its traditional uses for centuries and reports in literature.
Health Benefits
Digestive: Clove aids digestion by stimulating the secretion of digestive enzymes. It is also used to alleviate flatulence, gastric irritability, dyspepsia, and nausea. Roasted powdered clove is usually taken with honey as a remedy to relief digestive disorders. Antibacterial: Clove found to have 29 phytochemicals with antibacterial properties against a number of pathogens including specific bacteria that spreads cholera. Anti-carcinogenic: Clove really attracts the attention of scientists for its anti-carcinogenic properties. A study demonstrated that clove may be helpful in controlling lung cancer in its early stages. Hepatoprotective: Metabolism, in the long run, results in increased free radical levels. Antioxidants prevent free radical induced tissue damage by preventing the formation of radicals, scavenging them, or by promoting their decomposition. Clove offers a high amount of antioxidants which may be beneficial in protecting organs from the detrimental effects of free radicals, including the liver. Anti-diabetic: Consuming cloves on daily basis may be beneficial in regulating blood sugar in diabetics. A study has revealed that clove extract imitates insulin in certain ways and help in controlling blood sugar levels. Anti-osteoporotic: Phenolic compounds in clove such as eugenol and its derivatives, and bioflavonoids including flavones and isoflavones have been particularly found to be helpful in preserving bone density and the mineral content of bone, as well as increasing tensile strength of bones. Anti-Mutagenic: Mutagens is defined as chemical compounds that change the genetic makeup of the DNA by causing mutations. Biochemical compounds found in cloves such as phenylpropanoids shown to have anti-mutagenic properties. When administered to cells treated with mutagens, they were found to be able to control the mutagenic effects. Immunostimulant: A study showed that clove essential oil stimulated the immune system by increasing the white blood cell count, thereby improving delayed type hypersensitivity. The study also demonstrated that it restored cellular and humoral responses in cyclophosphamide-immunosuppressed mice in a dose-dependant manner. Hypocholesterolemic: One clove study found that a daily dose of cloves lowered cholesterol while improving insulin performance.
Antiviral: Dr. James A Duke in his ethnobotanical database shows that clove contains 21 phytochemicals that may act as antiviral. Taking clove tea either alone or combined with other antiviral herbs such as thyme, rosemary, cinnamon or neem may help in shortening of the flu or colds duration.
Reverse atherosclerotic plaque Speaking about cholesterol-lowering and antioxidant properties of clove, I would like to share a little tip on how to possibly reverse atherosclerotic plaque in arteries in our body especially those located in the brain, heart, penis and feet. Take 1 teaspoon of clove powder, 1 teaspoon of ghee or pure butter along with 1 teaspoon of pure pomegranate juice. Pomegranate syrup may also be used. Traditional uses Clove either alone or combined with other herbs can be used traditionally to treat candidiasis, bad breath, toothache, wounds, dental abscesses, muscle sprains, painful ejaculation, cholera, gingivitis, cold, cramps, cough, bloating, gastroenteritis, emphysema, diabetes, osteoporosis, stye (hordeolum), acid reflux, attitude sickness, typhoid, scanty menses, flu, grey hair, insect bites, entamoeba, schistosomiasis, sore throat, asthma, stomachache, headache, nausea, vomiting, fever, indigestion, and coryza.
Other traditional uses include relieving diarrhea, pneumonia, premature ejaculation, fatigue, lower back pain, sinusitis, phlegm, headache, hematemesis, acid reflux, bronchitis, irritable bowel syndrome, dizziness, and yellow teeth.
Note: Most of the traditional uses of clove in the aforementioned list can be found by browsing various alternative healing websites owned by Indian herbal practitioners or holistic health advocates.
Most of us forget names, dates or places from time to time. But Hilary Doxford never did. While the rest of us smile about our common inadequacy, she knew she was experiencing a genuine malfunction of her high-performance brain. “I did have a really good memory and didn’t need to write things down,” she says. “And I used to be able to multiply two four-digit numbers together almost instantaneously.” But one day, she started getting the sums wrong.
The doctors sent her away at first. So you can’t remember names or multiply 3,765 by 1,983 any more? Oh well, that’s middle age for you. But Doxford, who was then in her late 40s, knew differently. “My benchmark is myself,” she says. “Even now, when I tell people, everybody says: ‘I would never have known.’ What I’m doing is no different from what other people are experiencing. But when I compare it to how I used to be … I can’t multiply a two-digit number by a one-digit number. I can do it if I add them – like 27 times three. It’s my short-term memory – when you need to hang on to a number because you need to use it. That’s what’s gone.”
Doxford went to the GP because her partner, Peter, had asked her to marry him. She wanted to be sure she would not be sentencing Peter to looking after a woman whose brain was deteriorating. “My GP said: ‘It’s normal – off you go.’”
Three years later, then a married woman, she went back. “All the symptoms were getting worse,” she says. Doxford is the general manager of a medical research charity.“I forgot the surnames of some of my staff. I started finding it hard to concentrate and focus. Then I started avoiding taking responsibility for things unless I absolutely had to.”
The GP said it was probably stress and sent her home again. But then she had a long, difficult business meeting with somebody, and when he greeted her three weeks later, she had no recollection of having met him before. This time she was sent for tests. She scored incredibly highly on the IQ part and incredibly poorly on memory, and was given an MRI scan. “The diagnosis was Alzheimer’s,” she says, matter-of-factly.
‘My benchmark is myself. When I compare it now to how I used to be’ … Hilary Doxford, who was diagnosed with Alzheimer’s in her early 50s. Photograph: Lydia Goldblatt for the Guardian
Dementia will take hold of one in three people who passes the age of 65, and costs the UK more than £26bn a year. This week the Office for National Statistics announced it is now the commonest cause of death in England and Wales, passing cancer and heart disease. People with dementia lose the ability to care for themselves and can become malnourished, while their immune system weakens. Infections such as pneumonia may be the actual agent of death, but dementia is the underlying cause.
It is a cruel disease, which takes away the person their families love and know, leaving a stranger who looks at them with confusion. And while there are are some drugs that will temporarily alleviate symptoms in some people, there is no cure. But dementia, of which Alzheimer’s is the commonest form, has finally begun to get the attention it deserves. In December 2013, the G8 countries, meeting in London, agreed to set an ambition to cure or come up with a significant treatment for Alzheimer’s by 2025. Last year David Cameron announced that the UK would set up a dedicated dementia research institute, with initial funding of £150m, and a further £100m from Alzheimer’s charities. Although the UK was already spending £300m on dementia research, Cameron believed it should be afforded the same level of resources as Aids and climate change. That was welcome news to campaigners, although, they say, the sum is still much less than that invested in cancer research (£590m in 2010).
Doxford, now 56, was glad to have a diagnosis. “On the one hand, it was a relief, because it explained all the problems I’d been having just doing normal stuff. On the other hand, ‘Oh shit’. The first question I asked the consultant was: ‘How long have I got being normal?’ He was implying that I only had two to three years, but then he said: ‘I do know somebody who is eight years down the line and she is pretty much OK.’” Others Doxford has met have since told her of people managing fine 10 to 15 years after diagnosis. For her, it has now been nine.
Initially she was put on Aricept (the brand name of donepezil), one of the few Alzheimer’s drugs currently available. These drugs help some people by delaying the worsening of symptoms, although they progress faster later on. But they do not work for everyone.
“It was pretty horrendous,” says Doxford. “I seemed to get all the side effects on the packet.” She began falling over. The worst was when she was tying up the boat that she and her husband kept. “We were in the marina and I had the rope in my hand. The next thing I knew, I was in the water.” They sold the boat, fearing for her safety. The consultant gave her another drug, but it was worse. “The first day I took it, I thought I was dying,” she says. She decided drugs were not for her.
There ought to be big money in Alzheimer’s drugs. It is more than a century since abnormal protein deposits in the brain were identified by the German psychiatrist Alois Alzheimer as a likely cause of neurodegeneration. Over the past few decades, drug research has focused largely on attempts to clear the amyloid-beta peptides and tau proteins believed to cause these deposits, which gradually shut down the brain’s normal workings.
But there has been a very high failure rate, often at a late stage of development, when companies have spent a great deal of money – in some cases as much as $ 300m – on research and development. Dr Eric Karran, formerly the director of research at Alzheimer’s Research UK and now leading the efforts of drug company Abbvie to find a cure, says that yes, it’s difficult, but too often in these failed trials, the preparatory work has not been thorough enough.
“Some people in the field would say that [the failure rate] has been a disaster,” he says. They suggest that the underlying concept, that Alzheimer’s is caused by amyloid plaque, may be wrong. “I would not subscribe to that view. There has been some sloppy science. We would not expect such trials to work anyway. In some cases there has been a very strong commercial push. In other cases, there has been a strong desire to get something into [human trials] because we have so little.”
Nobody would say research into Alzheimer’s is easy, says Dr Mike Hutton, chief scientific officer for neuroscientific drug discovery at the pharmaceutical company Lilly. “Amyloid accumulates in the brain for 10 to 15 years before you see clinical symptoms. There is a worry that we’re focusing on populations that are too far advanced.” Ideally, scientists must figure out who is most likely to get Alzheimer’s – then see if they can prevent healthy brains from developing it. But although there are some predictive tests available, it is hardly ethical to offer them to people when medical science cannot offer them treatment.
So the trials must be done in people with the earliest stages of dementia. And this year, for the first time, the results of two separate early trials have suggested that it may be possible to find drugs that might slow down the decay for people with mild dementia. Small wonder there have been wild headlines about a cure – a bit of good news is desperately wanted. One, Lilly’s solanezumab, a monoclonal antibody, failed in a large 2012 trial to slow the deterioration in most people with Alzheimer’s, but there was some improvement in those with the mildest form of the disease. Results from a new trial of more than 2,000 people with early-stage Alzheimer’s are eagerly anticipated, and due before the end of the year.
Another drug, Biogen’s aducanumab, made headlines in September. Trial results showed it almost completely cleared amyloid from the brains of a group of early Alzheimer’s patients,and that the expected deterioration slowed down significantly. The trial was small (166 people), and at the high doses that produced the best results, there were side effects such as headaches, but there was excited talk of “a game-changer”.
There has been such hype before, but David Reynolds, chief scientific officer of Alzheimer’s Research UK, says he is reasonably confident that the solanezumab results in December will also show an improvement in the symptoms of dementia, or at least a slowing of the decline. Sadly, there still seems little hope for those who already have moderate to severe dementia, beyond care and compassion.
In a nursing home in Hertfordshire, surrounded by trees and green spaces, James Gatesman, a former coroner’s officer and enthusiastic allotment gardener, spent the last years of his life in bed, his long legs angled to the wall, under a framed photograph of his Metropolitan police class at Hendon College. A yellow spot attached to the glass identified his own face in the picture.
Deborah Gateman with her father, James, before he died. Photograph: Lydia Goldblatt for the Guardian
You could still see the fine figure of a man that Gatesman had been – 6ft 2in with broad shoulders and a strong, handsome face. But he had ceased to speak, and could no longer move his own limbs. His daughter Deborah and his wife, Doreen, could only communicate with him through touch, or his occasional grunts, moans and howls.
“I always talk to him and treat him as if he understands us,” said Deborah, shortly before her father died. “I think of it as almost like locked-in syndrome – that he is in there. I worry about what we discuss in front of him.” When his wife paid for him to have music therapy, Gatesman responded to the Gilbert and Sullivan tunes he used to love with noises and movement of his hands. That confirmed Deborah’s belief that he was more aware than he seemed.
Gatesman was diagnosed in 2003, but Doreen recalls odd behaviour on a holiday in Australia in 1996, when he wandered away from their group and nobody knew where he was. In later years, his behaviour became unpredictable, and he refused to go to a doctor. “That was probably the worst time,” she said. “Where do you go for help?”
Eventually Gatesman had to see a GP because of an ear infection, and ended up in the memory clinic. He had a brain scan and was diagnosed with Alzheimer’s. The progression was slow but inexorable. He was on Aricept for a year, but that was stopped when he was sent to a residential assessment centre – a care home where people with dementia spend some weeks or months while their condition and needs are determined. Instead, he was put on the drugs that are too often used to control the sometimes bizarre and agitated behaviour of dementia patients – antipsychotics. “He was throwing chairs around and he did pull a handrail off the wall,” Doreen says. When they visited him, he was no longer walking, but sitting in a reclining chair. “He was a bit of a dribbling mess,” said Deborah. “The antipsychotics were turning him into a zombie.” By the time he was moved to the long-term home in Hertfordshire, he was underweight. Doreen insisted the antipsychotics were stopped, and he regained not just his weight, but his spirit. Then “they had quite a lively character on their hands. He would run off down the corridors,” said Deborah. Or he would speak to the Polish nurses in the Flemish and German he had learned while in the RAF, in the war.
The Alzheimer’s Society has campaigned to reduce the use of antipsychotics – often referred to as the “chemical cosh” – in care homes. Dr Doug Brown, the organisation’s research director, says prescriptions have markedly reduced as a result, though “we wouldn’t say the problem has gone away. We still need to keep an eye on it”. The Society has piloted staff training in more than 100 care homes for “person-centred care”, which appears to cut the use of drugs dramatically. It involves taking the trouble to understand the triggers for an individual’s distress – such as the man who gathered all his furniture in the centre of his room every day and became upset when staff put it back. He was a decorator. Given a brush and a bucket of water, he spent contented hours thinking he was painting the walls.
The overuse of antipsychotics is one outcome of the past neglect of dementia, and further evidence of the real need for a drug that will do more than just quieten patients down – one that will slow the progress of a devastating disease and eventually, hopefully, cure it.
Gone are the days of clunky wheelchairs seemingly designed to hinder as much as to help – at least for some. The latest promising development in the disability world comes from ex-Royal Marine Phillip Eaglesham, who was almost paralysed after contracting Q-fever on his last day in Afghanistan. When he began to lose strength, he used a Segway to get around and realised how helpful its versatility was. Now that he cannot use one, he has designed a new chair that copies some of the Segway’s features to allow wheelchair users to manoeuvre easily and, most importantly, raise themselves up to eye-level and have a decent conversation.
My electric wheelchair is nowhere near as cool, but I can raise myself to just below standard eye-height. It’s hard to express how much this helps me have a normal life. Yes, of course it means that I can reach things on shelves and whatnot. But it also means I can do typical twentysomething activities such as introduce myself in a noisy environment or even, God forbid, sit at a bar.
Without it, crowded places such as clubs become a nightmare, as does meeting new people. People are conditioned to notice others of a standard height and to patronise those whose heads are more at the level of a child’s. My cerebral palsy makes it hard to project my voice, so being able to raise myself up allows me to engage with others as an equal.
Yet the relevant authorities do not believe that features such as this are important. The NHS wheelchair service will only provide wheelchairs that meet medical needs; independence and social needs are ignored. The result is that decent wheelchairs, and by extension a decent quality of life, are reserved for those who can afford them – and they can be prohibitively expensive. The new design is projected to cost a tidy £10,000.
My friend Anna has spinal muscular atrophy, and relies on a highly specialised chair that can transform into a standing frame to help retain her muscle strength. Last year her old chair malfunctioned – throwing her to the ground, leaving her with sprained ankles. Since then, while she fundraises for a replacement, she has been given a manual chair that she cannot move at all, and a borrowed powerchair that does not meet her needs. The model she needs, that will allow her to go about her daily life, costs £24,000. The NHS provided a voucher for £1,295, the cost of its standard chair. This barely makes a dent in the total sum needed. Over a year later, Anna is finally ready to order the right chair. Others may not be able to work so hard to raise money.
For some disabled people, our wheelchairs are the substitute for our legs. Yet the way we treat disabled people is like asking someone who has broken both legs to pay for the operation to fix the second break – and this from a government that aims to get more of us in work, while remaining indifferent to helping us do so.
Inventions like Eaglesham’s have the potential to make disabled people’s lives much better. But with so many people unable to access a chair that is even remotely suited to their lives and needs, progress seems far off. As technology improves, the possibility of better equipment grows, but so does the gap between those who can and cannot afford it. Only the state can level this cruel inequality.
First, the myths. There are no “super rats”. Apart from a specific subtropical breed, they do not get much bigger than 20 inches long, including the tail. They are not blind, nor are they afraid of cats. They do not carry rabies. They do not, as was reported in 1969 regarding an island in Indonesia, fall from the sky. Their communities are not led by elusive, giant “king rats”. Rat skeletons cannot liquefy and reconstitute at will. (For some otherwise rational people, this is a genuine concern.) They are not indestructible, and there are not as many of them as we think. The one-rat-per-human in New York City estimate is pure fiction. Consider this the good news.
In most other respects, “the rat problem”, as it has come to be known, is a perfect nightmare. Wherever humans go, rats follow, forming shadow cities under our metropolises and hollows beneath our farmlands. They thrive in our squalor, making homes of our sewers, abandoned alleys, and neglected parks. They poison food, bite babies, undermine buildings, spread disease, decimate crop yields, and very occasionally eat people alive.A male and female left to their own devices for one year – the average lifespan of a city rat – can beget 15,000 descendants.
There may be no “king rat”, but there are “rat kings”, groups of up to 30 rats whose tails have knotted together to form one giant, swirling mass. Rats may be unable to liquefy their bones to slide under doors, but they don’t need to: their skeletons are so flexible that they can squeeze their way through any hole or crack wider than half an inch. They are cannibals, and they sometimes laugh (sort of) – especially when tickled. They can appear en masse, as if from nowhere, moving as fast as seven feet per second. They do not carry rabies, but a 2014 study from Columbia University found that the average New York City subway rat carried 18 viruses previously unknown to science, along with dozens of familiar, dangerous strains, such as C difficile and hepatitis C. As recently as 1994 there was a major recurrence of bubonic plague in India, an unpleasant flashback to the 13th century, when that rat-borne illness killed 25 million people in five years. Collectively, rats are responsible for more human death than any other mammal on earth.
Humans have a peculiar talent for exterminating other species. In the case of rats, we have been pursuing their total demise for centuries. We have invented elaborate, gruesome traps. We have trained dogs, ferrets, and cats to kill them. We have invented ultrasonic machines to drive them away with high-pitched noise. (Those machines, still popular, do not work.) We have poisoned them in their millions. In 1930, faced with a rat infestation on Rikers Island, New York City officials flushed the area with mustard gas. In the late 1940s, scientists developed anticoagulants to treat thrombosis in humans, and some years later supertoxic versions of the drugs were developed in order to kill rats by making them bleed to death from the inside after a single dose. Cityscapes and farmlands were drenched with thousands of tons of these chemicals. During the 1970s, we used DDT, the active ingredient in Agent Orange. These days, the poison is not just sown in the earth by the truckload, it is rained from helicopters that track the rats with radar – in 2011 80 metric tonnes of it were dumped on to Henderson Island, home to one of the last untouched coral reefs in the South Pacific. In 2010, Chicago officials went “natural”: figuring a natural predator might track and kill rats, they released 60 coyotes wearing radio collars on to the city streets.
How is it that we can send robots to Mars and yet remain unable to keep rats from threatening our food supplies?
Still, here they are. According to Bobby Corrigan, the world’s leading expert on rodent control, many of the world’s great cities remain totally overcome. “In New York – we’re losing that war in a big way,” he told me. Combat metaphors have become a central feature of rat conversation among pest control professionals. In Robert Sullivan’s 2014 book Rats, he described humanity’s relationship with the species as an “unending and brutish war”, a battle we seem always, always to lose.
Why? How is it that we can send robots to Mars, build the internet, keep alive infants born so early that their skin isn’t even fully made – and yet remain unable to keep rats from threatening our food supplies, biting our babies, and appearing in our toilet bowls?
“Frankly, rodents are the most successful species,” Loretta Mayer told me recently. “After the next holocaust, rats and Twinkies will be the only things left.” Mayer is a biologist, and she contends that the rat problem is actually a human problem, a result of our foolish choices and failures of imagination. In 2007, she co-founded SenesTech, a biotech startup that offers the promise of an armistice in a conflict that has lasted thousands of years. The concept is simple: rat birth control
The rat’s primary survival skill, as a species, is its unnerving rate of reproduction. Female rats ovulate every four days, copulate dozens of times a day and remain fertile until they die. (Like humans, they have sex for pleasure as well as for procreation.) This is how you go from two to 15,000 in a single year. When poison or traps thin out a population, they mate faster until their numbers regenerate. Conversely, if you can keep them from mating, colonies collapse in weeks and do not rebound.
Solving the rat problem by putting them on the pill sounds ridiculous. Until recently no pharmaceutical product existed that could make rats infertile, and even if it had, there was still the question of how it could be administered. But if such a thing were to work, the impact could be historic. Rats would die off without the need for poison, radar or coyotes.
SenesTech, which is based in Flagstaff, Arizona, claims to have created a liquid that will do exactly that. In tests conducted in Indonesian rice fields, South Carolina pig farms, the suburbs of Boston and the New York City subway, the product, called ContraPest, caused a drop in rat populations of roughly 40% in 12 weeks. This autumn, for the first time, the company is making ContraPest available to commercial markets in the US and Europe. The team at SenesTech believes it could be the first meaningful advance in the fight against rats in a hundred years, and the first viable alternative to poison. Mayer was blunt about the implications: “This will change the world.”
Mayer is a tall, vigorous woman in her mid-60s with bright eyes, spiky grey hair and a toothy grin. Her ideologies of choice are Buddhism and the Girl Scouts. “It’s kind of my core,” she said of the latter, “to do for others.” In conversation, her manner is so upbeat that she seems to be holding forth radiantly before an audience or on the verge of bursting into song. When asked how she is doing, she frequently responds in a near-rapture: “If I was any better, I’d be a twin!” – she also appears to enjoy watching people wonder whether this is an expression they should know.
When I took a seat in her office earlier this year, she clapped her hands triumphantly and said “Ooh! You’re sitting in history and strength!” There was a pause. “I had a feng shui person come and do my office,” she explained.
Loretta Mayer, CEO of SensTech, holds up a test cup of the company’s rat contraceptive formula. Photograph: Taylor Mahoney/SenesTech
Mayer came to science later than usual, in her mid-40s, after a career in real estate development and a stint as the international vice president of Soroptimist, a global volunteer organisation dedicated to improving the lives of women. The career change was unexpected, even to her. After a close friend died suddenly of a heart attack, Mayer called up a biologist she knew and asked how something like this could have happened. The biologist had no satisfying answer; she explained that while heart disease in men had been thoroughly studied, little attention had been devoted to post-menopausal heart disease in women. “Well you’ve got to change it,” Mayer replied, outraged. The biologist was otherwise occupied, so Mayer decided to do it herself. At 46, she entered a PhD programme in biology at Northern Arizona University.
After graduate school, her initial research as a professor of biology at Northern Arizona focused on artificially inducing menopause in lab mice so that she could study changes in the postmenopausal heart. Three years into her efforts, Mayer was contacted by Patricia Hoyer, a colleague in Phoenix, who said that she had stumbled across a chemical that seemed to make mice infertile, without having any other effects. Together, Mayer and Hoyer synthesised a new compound, which they called Mouseopause.
Shortly after Mayer and Hoyer published their work on Mouseopause in 2005, Mayer received a telephone call from a veterinarian in Gallup, New Mexico, who had read about her research. The Navajo reservation where he worked was overrun by wild dogs. There were too many to spay and neuter, so he was euthanising almost 500 a month. “If you could do for a dog what you can do for a mouse, I could stop killing dogs out here,” he told her.
Mayer describes herself as “extremely connected to animals, dogs in particular”. When she arrived in Gallup and saw the piled corpses, she agreed to test Mouseopause on an initial group of 18 reservation dogs. “I held up that first puppy, who I called Patient Zero,” she told me, “and I said, ‘I don’t know what this is gonna do to you, but you will live on a satin pillow the rest of your days.” The injection made the dogs infertile, but left them otherwise happy and healthy. (Mayer brought home all 18 dogs and built a kennel in her yard to house them until she could find homes for them with families she knew personally. Patient Zero, renamed Cheetah, lived with her until she died of old age – though the pillow was fleece.)
The next call came from Australia in 2006. Biologists there wanted an adaptation of Mouseopause for rats. Rats, they told her, were eating 30% of the rice crop in Australia and Indonesia. If she could reduce the rat population by even half, they claimed, the crops that would be saved could feed millions of people.
Mayer was moved by the idea of finding a solution to rat overpopulation that was neither lethal nor toxic. Since its invention, rat poison has been our primary method of curbing rat populations, but it is dangerous. Ingested in high doses, it’s fatal to humans, and it poses a particular to children because it is sweet and brightly coloured. In the US alone, more than 12,000 children per year, most of whom live below the poverty line, are accidentally poisoned by pesticide meant for rats.
The collateral damage inflicted by rat poison also extends to the environment, leaching into the soil and poisoning house pets, farm animals, and wildlife that feed on rats. Worst of all, rat poison is not very effective at eliminating large infestations. As long as there is still a food source, colonies bounce back, and, especially in Europe, rats have grown resistant to the toxins. As Mayer often says, “Doing the same thing over and over and expecting different results: isn’t that the definition of insanity?”
Persuaded by the research, and by her wife, fellow biologist Cheryl Dyer, Mayer decided to devote her career to developing a new, smarter way to control the rat population. In 2007, they founded SenesTech. “People say never to invest with a husband and wife team,” Mayer joked to me. “I say, ‘Oh absolutely not! Then you have dominance.’ But wife and wife? Works great!”
For Dyer and Mayer, the immediate problem was obvious: while the lab mice and feral dogs had received injections in controlled studies, wild rats would have to eat the formula of their own volition. Rats are neophobic – they avoid what they don’t know. What’s more, city rats are already well fed. In New York City, for example, they have fresh bagels, pizza, melted ice cream and fried chicken in unending supply. To succeed, Dyer and Mayer had to make the compound not just edible but delicious.
After a series of tests, they quickly settled on a liquid, rather than solid, formulation. Rats have to drink 10% of their body weight every day to survive, and so are always looking out for something potable. “We compared the [two] and they peed on the solid and drank the liquid,” Dyer told me. “Rats are pretty straightforward.”
Where Mayer is tall and voluble, Dyer is short and broad-shouldered, quiet and succinct. She seems most comfortable behind the scenes, if only because it is easier to get away with wearing Hawaiian-print shirts and no shoes. At SenesTech’s headquarters, Dyer’s windowless office is right next to Mayer’s, and if Mayer’s office evokes Zen, Dyer’s evokes an island paradise. Scenes from Hawaii cover her walls, hula (and rat) figurines line the shelves, and on her desk sits a small wooden sign, which says, “WELCOME TO THE TIKI BAR.” There is also a widescreen TV, on which Dyer likes to watch old movies on mute all day.
It was Dyer’s job to make Mouseopause palatable for rats – a tricky proposition because its active ingredient, 4-vinylcyclohexene diepoxide (VCD), is bitter and caustic. Rats have the same taste preferences as humans – they love fat and sugar – though Dyer’s experiments with various flavour profiles indicated that their appetite for both exceeds ours.
She was also tasked with the greater challenge of adapting Mouseopause to work on rats, which are much hardier than mice. While VCD caused the eggs in mouse ovaries to degenerate rapidly, female rats were far less susceptible. Hoping for a compound effect, Dyer added a second active ingredient: triptolide, which stunted any growing eggs. The results were better, but still not good enough. “They just had smaller litters, goddammit,” she said.
Eventually, out of a mix of curiosity and desperation, she fed it to both males and females. The result was dramatic. It turns out that the triptolide destroyed sperm – the males became sterile almost immediately after ingesting the formula. This was a total surprise: no one had ever tested triptolide on male rats before. It was “stunning”, Dyer told me. “Totally unpredictable.” Test after test: no pups. She sighed. “Man, you should have seen the No Pup party.” After three years of research and development, they had a product that worked and did not harm other animals. (The active ingredients are metabolised by the rat’s body in 10 minutes, which means that any predator that eats it is not affected, and the compound quickly breaks down into inactive ingredients when it hits soil or water.)
ContraPest, the finished product, is viscous and sweet. Electric pink and opaque, it tastes like nine packets of saccharine blended into two tablespoons of kitchen oil. “Rats love it,” Dyer said. “Love it.” Mayer, who taste-tested every version during the development process, could not say the same for herself.
In 2013, New York’s Metropolitan Transit Authority (MTA) reached out to Mayer after hearing about SenesTech’s early trials to ask whether the company would test ContraPest in New York’s subways as part of a citywide effort to find new, more successful alternatives to poison. Many cities devote manpower and money to keeping the rats under control, but New York, which is more or less the rat capital of the western world, is the epicentre of anti-rat efforts. Every incoming mayor of New York declares his intentions for a vast rodenticide – Giuliani even appointed a “rat czar” to oversee the carnage – only to leave the next guy even more to deal with.
Brown rat (Rattus norvegicus) rearing up. Guardian Design Photograph: Frank Greenaway/Getty Images/Dorling Kindersley
When the MTA officials contacted Mayer, she recalled, they were worried that the formula would not work on New York rats, which have the reputation of being bigger, tougher, and smarter than any other city rat in the world. (Norway rats, the species infesting New York, are not in fact the largest rat type.) They asked Mayer whether they should send a few New York rats on a plane to Arizona so that SenesTech could experiment with them before coming to New York. “No, I don’t think so,” replied Mayer, amused. “I never met a rat I couldn’t sterilise.”
Mayer dispatched two of SenesTech’s youngest scientists, women in their 20s, to New York in order to test whether the formula was appealing enough. Would New York rats prefer ContraPest to water or pizza? Wearing their best approximation of hazmat suits to protect themselves from the filth, the scientists patrolled the subway’s trash storage rooms under Grand Central Station. They planted bait boxes filled with feed stations of ContraPest and then stood nearby, counting the rats that came in and out with clickers in order to track how many rats were taking the bait. For six months, they baited and counted, washing their suits at the end of each day in bleach.
The two young women went home to Arizona with good news: not only did the New York rats drink ContraPest, the drink actually worked on them. The test confirmed the highest hopes of the company – there was an alternative to poison that would work, even in New York City, and they had found it.
When humans and animals come together, there are choices. Mayer believes that if you understand the ecology of the animal and you understand your own ecology, then you and the animal will be able to coexist peacefully. After centuries of misperception and squeamishness, we finally have a good grasp of rat ecology. Now the problem may be our reluctance to look too carefully at ourselves.
In his 1983 book More Cunning than Man, writer Robert Hendrickson lists “the obvious ways in which rats so well resemble humans: ferocity, omnivorousness, adaptability to all climes, migration from east to west in the life journey of their species, irresponsible fecundity in all seasons, with a seeming need to make genocidal war on their own kind.” He describes rats and men alike as “utterly destructive, both taking all other living things for their purposes.”
Humanity’s long struggle with rats mostly signals the worst traits we share with them: our inability to live responsibly within our environment; our tendencies toward hedonism and greed; and our failures to look after the weakest among us. Getting rid of them means correcting ourselves first.
SenesTech is not alone in its attempts to devise a more sustainable, responsible method of ending the rat problem. Its work is heir to an existing method: integrated pest management, or IPM, which holds that if humans – particularly city-dwellers – took more care with their environment, rats wouldn’t thrive.
IPM’s most vocal advocate is Bobby Corrigan, who has brought its principles to farmlands and cities all over the world, most notably New York, which recently revised its rat control programme on his advice. Twice a year, he teaches the New York health department’s “Rat Academy”, a three-day training for industry professionals. This April, there were maybe 100 attendees wedged into wooden theatre seats in a downtown auditorium, holding weak coffee and spongy muffins.
Corrigan is a thinnish, pale man, bald except for a low, wispy crown framing his ears. He spends his nights on the streets or in basement corners studying rats. Once, he lay in an alley with peanut butter spread around him all night so he could get good photographs. (“No, it wasn’t safe. Yes, they were urinating on me. In grad school, you do crazy things.”) He regards his work with utmost seriousness.
“Here’s what health professionals do,” he said to his audience by way of introduction. He pointed at a slide behind him and read aloud.
We protect the roof over people’s heads. We protect the food they eat. We protect their health, comfort and safety.
“I’m not saying this to pat us on the back. This is real. This is our job. [Rats] get on airplanes. They gnaw on wires. They cause diseases. To me, this is the shot heard round the world.” Then he spent 20 minutes explaining how to divine information from rat droppings based on their moisture.
As the day wore on, Corrigan’s core message for his audience emerged: fighting rats means committing to holistic efforts, not looking for a quick, flashy fix. “We love to spritz problems away,” Corrigan told me later. “A chemical or a trap, it’s a Band Aid, and they’re Band Aids that come off very quickly.” Instead, Corrigan argues that you first need to remove the rat’s food, then remove the rat’s shelter, and only then take lethal measures if you have to.
In theory, this solution is simple. It does not involve radar or guns. Instead, it demands lids for the trash can, and caulking for the cracks in foundations, or “keeping our own little nests clean”, as Corrigan says. It is the obvious answer, the one that has been sitting under our noses for centuries: stop feeding them, stop housing them, and they will go away on their own.
The problem is that people, as a rule, prefer the quick fix. Setting out poison is easier; the ultrasonic machine looks cool. The sensible, labour-intensive option meets with resistance. Often, when Corrigan is called out to consult with a property owner, the owner rejects his advice, simply because following it would require too much thought, effort or expense.
Your rats are my rats. If the city blows it off, the sewer rats become everybody’s rats. Rats are everybody’s issue
And sometimes, even those who are willing to try his methods do not have the resources. Ricky Simeone, the director of pest control for New York’s health department, explained to me that the neighbourhoods that struggle with the worst rat infestations are not the ones who file the most reports to his office. The poorest neighbourhoods are too overwhelmed with other social or economic problems to file complaints – or, worse, they accept rat infestation as one of the conditions of living in poverty.
Corrigan confirmed that rats, especially in cities, affect the poor more than the rich, because effective pest control services are expensive. But he pointed out that no one totally escapes the rat problem, no matter how rich. Cities such as New York make evident a universal truth. “We’re all holding hands whether we know it or like it. Your rats are my rats. If the city blows it off, the sewer rats become everybody’s rats. Rats are everybody’s issue.
“Everyone thinks, ‘It’s not my job, it’s someone else’s job,’” Corrigan continued. “They think, ‘Oh I live in New York, no one can get rid of the rats in New York!’” He gave a short sigh. “We don’t think we can do it alone, so we don’t do anything as a group.” As with all conditions that threaten everyone but torment the disadvantaged above all, the situation is not better because we are not better.
“Homo sapiens,” Corrigan said to his audience at the Rat Academy. “Does anyone know what this means?”
He smiled a grim little smile. “Wise man.”
Improving society is a collective project, but as Corrigan attests, it happens because individual people make it their business to incite change. Mayer and Dyer, too, see this as their mission. “We have to be better stewards than this,” Dyer told me fiercely. “We’re better than this.” If SenesTech looks quirky in the attempt, its founders do not seem to mind.
‘Rats are so longstanding a threat to humanity that contemplating an end to the rat problem seems like a fantasy.’ Photograph: AFP/Getty Images
On a Tuesday night in August, Mayer and Dyer held a celebration in their backyard for staff and investors. The company had just received US Environmental Protection Agency registration, a process that usually takes years and often costs more than companies of SenesTech’s size can afford. (The EPA is making an active effort to get rat poison off the markets in the US, and received news of SenesTech’s science with enthusiasm.) Now, with the EPA’s blessing, the company could take ContraPest to commercial markets. Immediately, more than 100 calls and 200 emails came in with order requests.
Mayer and Dyer live in a one-level wood cabin a few miles north of downtown Flagstaff, in a wooded area near a field of wildflowers. For the occasion, they had cleared the back patio, where Mayer does her morning meditation and yoga, and filled it with deck furniture and folding tables. The sun was coming down the San Francisco Peaks.
It was not a typical investors dinner, but then, SenesTech’s nearly 700 stakeholders are mostly firemen. While most biotech startups are funded by investment bankers and venture capitalists, Mayer chose to pursue funding from grant-giving bodies and a horde of private donors, all of whom made small investments, and each of whom Mayer knows by name. It was a pure accident of networking that so many of them turned out to be firemen, but she is thrilled with the situation. “Firefighters really believe in doing good,” Mayer explained to me. “And they’re like teenage girls. Once one of them invested, they all wanted in.”
There were perhaps 25 people – investors, board members and SenesTech staff – gathered on the back patio, eating tacos and drinking from Mayer and Dyer’s impressive liquor collection, but they made noise for 50. They were boisterous and loving, hugging each other, teasing each other, shouting old stories to roars of laughter, and clinking glasses. About half the room seemed to be wearing Hawaiian patterned shirts.
When the time came for Mayer to give a speech, she demurred for a moment before standing. Her toast turned briefly into an anecdote about flattening mouse skeletons in lasagna tins. “But seriously,” she said, returning to her theme, “We knew [this day] would come. It’s great to be riding this wave with you. It’s just so sweet.” Glasses heaved into the air.
There was considerable work left to do: now that SenesTech had its national registration, it would have to file for registration in every state. (Since then, the company has registered in 11 US states, and begun registration in the EU.) The manufacturing team was hurrying to make enough ContraPest to accommodate the requests coming in.Dyer was working hard on adaptations that would make the formula work in a variety of different environments, and planning variations for different species. Mayer was preparing for a torrent of meetings. While ContraPest has been effective in every test SenesTech has run so far, there is a lot still to learn about how rats in different parts of the world will respond to it in the wild.
It sounds crazy: a band of animal loversand firemen in the mountains of Arizona, led by a Buddhist girl scout, making a pink milkshake for rats that may eventually improve the lives of millions of people. They are unruffled by scepticism: In the middle of one interview, Mayer forgot a detail and yelled towards the door, “Cheryl, who said to you, ‘That’s just not how we do it?’” Dyer hollered back from the other room. “Which time?” In response, they point to hard science, solicitations from governments and companies around the world, and an endorsement from Stephen Hawking, who featured them on his documentary mini-series Brave New World.
Rats are so longstanding a threat to humanity that contemplating an end to the rat problem – and one that does not require us to kill them – seems like a fantasy. They are, as Mayer herself put it, a more successful species than us. Long after we’re gone, they will still be here. But the possibility of a truce seems closer than ever before. “The answer in the future may lie completely within biotechnology,” said Corrigan when I asked for his impressions. (He and Mayer consider themselves allies in the campaign to create sustainable solutions to the rat problem. Mayer fondly recalls a nighttime “rat safari” she once took with Corrigan in New York.) “The SenesTech product is a breakthrough, but it is still at the very infancy stages of biotechnology for this species,” Corrigan said. “This is going to be maybe years of refinements and changing and experiments. We’re not walking yet. And we’re certainly not running.”
Mayer, Dyer and their team seem cheerful at the prospect, and confident that they are doing the work of the future. “Do you see this?” asked Ali Applin, a senior member of SenesTech’s staff. We were sitting in Mayer’s office, and Applin pointed to a little sign on the coffee table that read “Make it so.”
“This is what she tells us,” Applin said.
Mayer nodded, smiling. “That’s what you need to do. I mean, why squabble over something and say, ‘I can’t do that’. Make it so. Find a way. There’s always a way.”
After a moment, she had another thought. “You’re really gonna have to do that, Ali, when you take this to Argentina soon. If we thought Laos was hard – I mean, my God.” She grinned mischievously and folded her hands together and pressed them to her forehead and said a mantra. “I wish you ease on the path to peace. I wish you an end to your suffering.”
• Follow the Long Read on Twitter at @gdnlongread, or sign up to the long read weekly email here.