Mental health problems in the prison population have long been a matter of concern. Suicide rates in prisons in England and Wales are at an all-time high; a record 119 people killed themselves in 2016 – an increase of 29 on the previous year, according to figures from the Ministry of Justice. The rise in prison suicides has been accompanied by a 23% increase in incidents of self-harm, to a total of 37,784.
“It’s a huge issue because lots of people in prison have mental health problems,” says Dr Steffan Davies, consultant forensic psychiatrist and co-chair of the Community Diversion and Prison Psychiatry Network at the Royal College of Psychiatrists. A study by the Prison Reform Trust found that 72% of male and 70% of female prisoners experience two or more diagnosable mental health disorders. Research by the National Institute for Health and Care Excellence found that 7% of male and 14% of female prisoners have a psychotic disorder – 14 and 23 times the level in the general population respectively.
The situation looks set to get worse. In recent years, staff numbers have dropped significantly, budgets and staff training have been cut, the prison population has more than doubled, and the introduction and rising use of new psychoactive substances has contributed to increasing violence.
Jacob Tas, chief executive of the social justice charity Nacro, says: “The overcrowded prison environment is likely to worsen existing mental health problems that are often the key drivers for offenders to commit further crimes or become violent while in prison.”
Davies adds: “It does feel like things are getting worse and I’m hearing it’s hard to recruit people to prison mental health services. People are leaving, and quite a few find it an extremely stressful environment to work in.”
While the general outlook is bleak, projects such as the self-management training programme at HMP & YOI Parc, Bridgend, south Wales, hold out some hope. Developed as a partnership between the Mental Health Foundation and G4S, and funded by Big Lottery Fund Cymru, the aim was to improve prisoners’ mental health through self-management and peer support.
The programme was delivered between September 2013 and December 2016, and involved two to three hours’ training one day a week for four weeks. Up to 10 participants could attend. Training included positive thinking, goal setting and problem-solving.
Fifty prisoners filled in the Warwick-Edinburgh mental wellbeing scale at the start of the course and a month after its completion: the mean score showed a significant increase in the prisoners’ wellbeing.
Lauren Chakkalackal, senior research officer at the Mental Health Foundation, says: “A number of positive stories came from the project. It was an opportunity for people to feel listened to and express how they were feeling.
“A group of prisoners produced resources to better support the mental health needs of new prisoners. The prisoners themselves took ownership of that group.”
Plans are afoot to develop similar models in other prisons and the project is being redesigned to support older prisoners and young offenders.
Our NHS is under attack from all angles. People are living longer, we don’t eat well or exercise enough. Yet we expect more from the NHS; more people are visiting A&E departments and minor injury units year on year, and costs are rising.
How do we tackle this? What if we focus on marginal gains, the performance strategy that helped British Cycling to success in multiple Olympics?
This is an approach that focuses on “small incremental improvements in any process adding up to a significant improvement when they are all added together”. Could this improve patient outcomes and reduce waste in the health service?
One incremental enhancement we could seek in the NHS might be to improve our understanding of and response to the barriers to patient motivation. For example, could we find a way of encouraging stroke survivors to practise their rehabilitation exercises as frequently and intensively as they are prescribed? Patient adherence to rehabilitation regimes after discharge from hospital is described as “less than ideal”. By addressing these barriers, we will be more able to efficiently allocate therapy time, and thereby reduce GP appointments and hospital readmissions.
You might wonder what makes me an expert on this.
Lowering patients’ expectations of recovery can be extremely damaging
In February 2010, at the age of 39, I had a huge brainstem stroke and was diagnosed with locked in syndrome. I was on life support and in intensive care for nine weeks, and was then written-offin rehabilitation after a further six weeks. My husband received a phone call telling him that I would never walk or talk again.
Over eight painstaking months in rehabilitation, I obsessively willed my body back to life, practising actions or movements 450 times per week. Slowly I learned how to do basic things like eat again, and at the end of it all I walked out of hospital. I went for a run on the first anniversary of my stroke. I’m now a motivational speaker and go to the gym every day.
[embedded content]
I never gave up pushing my body to improve: to speak, to eat, to run and to hug my kids. I managed to use my bad prognosis to galvanise my recovery, but the risk is that lowering patients’ expectations of recovery can be extremely damaging. Recovery should be measured in terms of improvements, not “getting better” – and that is always possible. My only focus, with three young children at home, was on when I would achieve my goals, not if.
Since embarking on my career in advocacy and stroke activism, I’ve found many reasons why patients lack the motivation to try to help themselves. They may be suffering from post traumatic stress disorder, which is common after a stroke and, just like depression, it affects mood and motivation levels. The side effects of the drug treatments for strokes – sleeping pills and muscle relaxants – can also affect motivation. After a brain injury many patients suffer varying levels of executive dysfunction affecting the set of mental skills that help to get things done, which can be mistaken for apathy or laziness. The overwhelming tiredness felt by those suffering from neurological fatigue can leave patients unable to complete normal daily tasks and therefore non-compliant with their treatment plans. It may be that some patients simply hate exercising or have no family support.
It is futile prescribing a stroke rehabilitation plan if – for any of these reasons – the patient is unmotivated before the therapy session starts or they are left at home trying to manage their own condition. The NHS should be offering hope and encouragement to motivate patients. And to do that, they need to listen to expert patients.
My advice to the King’s Fund Leadership Summit is that we need a better understanding of patient motivation to help rebuild the lives of stroke survivors. If patients adhere to clinical advice about practising their exercises as frequently and intensively as I did, just imagine how much we could improve their outcomes and reduce the waste in the NHS. But to do this we must understand the complex reasons why patients don’t do this already and listen to those who have struggled through similar experiences.
I don’t promise anything when I speak to people now – I just offer possibilities. I talk about how to optimise improvement, but never use the word recovery. After a life-changing event none of us will ever be the same as we were, even if we physically improve really well. We need to embrace that new self and strive to be the best version of ourselves that we can be, both in hospital and back home.
Join the Healthcare Professionals Network to read more pieces like this. And follow us on Twitter (@GdnHealthcare) to keep up with the latest healthcare news and views.
Among other weighty events on Wednesday, there is a chink of light that could transform the lives of thousands of people with learning disabilities, needlessly stuck in mental health institutions away from homes, families and communities. On Wednesday, the public affairs committee will hear from Simon Stevens, head of NHS England, and others, on reducing the number of people with learning disabilities in mental health hospitals to improve their quality of life. As a psychiatrist, I see many patients parked in hospital wards with years of their lives just rolling past. While the government’s target is to close 1,300 beds by 2019, only 60 beds have been closed so far.
Institutionalisation of this group of people in chaotic and turbulent hospitals for months, often years, on end can be devastating for their wellbeing. Yet this continues. Over 2,500 inpatients with learning disabilities remain in hospital, despite government commitment for them to have “the right to the same opportunities as anyone else to live satisfying and valued lives, and to be treated with dignity and respect … have a home within their community, be able to develop and maintain relationships, and get the support they need to live healthy, safe and rewarding lives”.
Discharging people from hospitals into community care transforms lives. A man, previously on my ward, self-harmed so severely and frequently that he blinded himself. When the right care package could eventually be arranged for his complex needs, he was discharged to residential care. The difference in his behaviour and quality of life is nothing short of breathtaking. Improving the lives of so many like him requires more than empty promises. Further specialist psychiatric input is needed to ensure people with learning disabilities are admitted to hospital only when it is the best place for them to be, and their care regularly reviewed so that they can return to the community as soon as they are ready. Dr Ashok Roy Chair of the Intellectual Disability Faculty, Royal College of Psychiatrists
• Join the debate – email guardian.letters@theguardian.com
• Read more Guardian letters – click here to visit gu.com/letters
Your article (Trump supporters in the heartland fear being left behind by GOP health plan, theguardian.com, 12 March) is unfortunately very consistent with a study that I recently commissioned looking at changes in white working-class death rates in California over the past 20 years. It showed that against a backdrop of improving white death rates in California, rural California is a veritable hot zone of white working-class mortality. Forty per cent of California counties (23 counties) voted for Donald Trump. Of those 23 counties, 21 of them are experiencing pronounced increases in death rates for whites aged 40-64. In some of these counties, white death rates have increased over 50% since the late 1990s.
This crisis of white premature death is being driven by alcohol and drug-related causes and includes a surge in suicides. These are the very types of health problems that are most amenable to high-quality mental health care and drug treatment services covered by Medicaid, which was expanded to millions of Californians under the Affordable Care Act. Our theory is that rapid shifts in the economy over this period without a meaningful social compact is the underlying cause of this epidemic of white death. These folks are watching the American dream slip further and further from their grasp and they are quickly losing hope. Tragically, their vote to repeal their healthcare access will likely exacerbate their pain. Dr Anthony Iton California Endowment, Oakland, CA, USA
• It’s reassuring to hear that Bernie Sanders is campaigning again (Journal, 11 March), but the examples given of his fightback are hardly likely to keep the light-sleeping President Trump awake at night. The usual emphasis on ever-more protests will soon meet the “too many marches” law of diminishing returns, as will I fear the hopes that his young supporters will still feel “the Bern” when the election is five years away rather than being imminent. His call for the Democrats to have a progressive platform geared more to the fears of steelworkers and less to the priorities of the liberal elites won’t on its own see off an increasingly authoritarian Trump. To do that it will need to include policies to cope with potential Democratic voters’ concerns about future immigration and to propose concrete steps to protect American jobs from imports.
This will require the Democrats to consider a progressive form of protectionism that will benefit all countries. Its core aim should be the nurturing and rebuilding of local economies not just in the US but worldwide. To adequately protect domestic jobs will need a permanent reduction in the level of international trade in goods, money and services and the prioritising of the ability of nation states to control the level of migration that their citizens desire. Without such an approach, Sanders could make more likely the ghastly prospect of an eight-year-long Trump reign. Colin Hines East Twickenham, Middlesex
• Trumps “Muslim ban 2” is planned to come into effect on Thursday 16 March. The ban, with very limited alterations, is just a repeat of the executive order that led to a global wave of protests. Islamophobia is at the heart of Trump’s agenda. The suspension of refugee programmes and the targeting of Muslim countries show just how far he is prepared to go to play divide and rule. We refuse to stay silent as Muslim communities are targeted and call on all those who oppose the ban to join us on the streets on Saturday 18 March as part of the global protests marking UN anti-racism day. Dr Shazad AminMend, Abra Javid Rotherham 12 Campaign, Rashid Majid KhanSolicitors, Amal AzzudinHuman rights activist,Tanzil ChowdhuryNorthern Police Monitoring Project, Nahella AshrafStand Up To Racism,Dr Amel AlghraniUniversity of Liverpool, Dr Waqas TufailLeeds Beckett University,Saleem AhmedBury Unison Black Members Officer,Maz SaleemDaughter of Mohammed Saleem,Sabia KamaliTV Presenter and Director of Sisters Forum, Vakas HussainBarrister, Zlakha AhmedFounder and manager of Apna Haq,Murad QureshiChair of Stop The War
• Rebecca Nicholson (Harry Potter and the Election of Horrors, G2, 14 March) tells an important story about the responses of Harry Potter fans to Trump’s election. She should certainly add to her account the case of the Harry Potter Alliance, the organisation of Rowling fans committed to acting out the values of non-discrimination and inclusiveness. But in just saying that each generation may have its effective “fictions”, she misses out the most important feature of this: that it is contemporary fantasy more than anything that is providing the means to this around the world.
It began with the Lord of the Rings films, which were accompanied for many by a picture of George W Bush wearing a gold ring with the slogan “Frodo has failed”. Then came Avatar, and the adoption of the Na’avis’ blue skin by environmental protestors. The Hunger Games provided anti-military protesters with the three-fingered salute of defiance. And of course Occupy borrowed heavily from V for Vendetta for its symbolism. But perhaps most interesting is the adoption by a number of anti-Trump protestors of the slogan “Winter is coming” from Game of Thrones. The difference being that on the face of it Game of Thrones is exceptional in being so dark and pessimistic. Yet it seems that it is helping people to feel hope within adversity. We are currently exploring this with our ongoing project, developed by 40 researchers in 12 countries. I hope some of your readers will be interested to visit, and perhaps contribute their views, at www.questeros.org. Martin Barker Emeritus professor, Aberystwyth University
• Join the debate – email guardian.letters@theguardian.com
• Read more Guardian letters – click here to visit gu.com/letters
In coming decades, rates of dementia will rise sharply, partly due to a “silver tsunami” as the boomer generation ages and partly because we are living longer than ever. By 2030, the WHO predicts 75.6 million people globally will have the disease.
In response, cities around the world are creating communities that better help people with dementia go about their daily lives (there are more than 200 such dementia-friendly communities in England and Wales alone).
This includes engaging businesses whose customers may have or be caring for people with dementia. “Making small changes in the way businesses and communities act can transform the quality of life and the contribution those with dementia and their carers can make,” says George McNamara, policy chief at Alzheimer’s Society.
Those small changes include training companies to recognise and support people with cognitive decline. In Bruges, for example, dozens of shops are designated as dementia friendly. Select employees are trained to recognise customers with the condition, allowing them to help those struggling to pay or find what they need, for example.
In Greater Manchester, taxi drivers are also being trained as “dementia friends” who recognise and assist customers with dementia, while in London, Lord’s cricket ground has created a project to reduce stigma and raise awareness. London recently announced a goal to become the world’s first dementia-friendly capital by 2020. Key areas of focus include (pdf) working with local health authorities to improve diagnosis rates and collaborating with Transport for London to make getting around safer and easier.
“If you get it right in cities you can have a big impact on a large number of people,” says Mark Drane, a Bristol-based architect and doctoral researcher with the WHO Collaborating Centre for Healthy Urban Environments. “And a city, in theory, has the levers to pull, especially for integrated care.”
Elsewhere, banks are training employees to help people with the dementia manage their money. HSBC, for example, has joined with Alzheimer Scotland and the Alzheimer’s Society in a three-year awareness raising partnership that has so far trained 2,000 UK staff across 742 branches.
In Southampton, British Gas is training staff as “dementia champions”, who can then teach other local business people and the public about the needs of those with dementia, holding monthly drop-ins to support people with the disease and their carers, and connecting staff to volunteer and fundraising opportunities in the community.
Around 7,000 of British Gas’s 30,000 UK staff are taking part in a dementia friends programme that trains them to be more informed about the illness.
Cutting costs
In addition to their work supporting customers, British Gas and Centrica are working to support employees who face dementia-related issues in their own lives. British Gas carers’ network, for example, offers a range of support, including giving employees flexibility to attend family members’ hospital appointments.
Centrica estimates that its caregiver support initiatives (paywall) save £2m in staff retention and potential training costs, and another £4.5m in preventing absenteeism of employees who are caregivers.
A 2014 report found that dementia costs UK businesses roughly £1.6bn per year, because of carers, more than half of whom are in work, having to reduce their hours or give up their jobs to look after a relative or friend with dementia. The Alzheimer’s Association estimates dementia costs US businesses $ 61bn (pdf), more than half of which it attributes to costs to businesses – including lost productivity – related to employees providing care.
As well as saving money through supporting employees, assisting customers with dementia offers businesses an opportunity to build and maintain their customer base. Sainsbury’s and the Federation of Small Businesses are among those that joined a federal retail task and finish group, which has produced a guide (pdf) on making shops dementia friendly. This isn’t merely corporate altruism: 83% of people with memory issues have changed where they shop based on how the business caters for people with dementia, according to the Alzheimer’s Society.
While a single company can have a significant impact locally, a multi-sector approach is crucial to creating dementia-friendly cities. Care City, for example, a research, education and innovation site in north-east London, works with the technology sector to develop products such as wearable devices for those with dementia.
Through NHS England’s healthy new town programme, Care City is also working with local communities to foster innovation in their backyards. That includes everything from an online platform where patients and their carers can log information about their health to a wearable location device that alerts carers if someone with dementia leaves a designated safe space.
Many projects currently begin in the health and social care system, or are driven by charities who work with businesses. In the future, more products and services to help people live at home longer and stay safe in their communities may come from industry itself.
According to McNamara, progress is being made by businesses, among others, to help those with dementia engage with their communities but there’s work to be done to ensure these ideas spread further. “Dementia,” he says, “is everyone’s business.”
Sign up to be a Guardian Sustainable Business member and get more stories like this direct to your inbox every week. You can also follow us on Twitter.
“I just need a letter to say I am fit to fly,” he says, my young patient who has gone from being a paragon of fitness to needing a walking stick in a space of only two years. Today, he is on an unscheduled visit, promising not to stay long, not that I mind. I’m fond of him and have grown to admire the way in which his family has coalesced at a difficult time. His wife left her job, his pregnant daughter has moved in to help, and his two sons are always around for appointments.
But fit to fly? I’m alarmed.
Fly to where? He is pale and gaunt, his eyes magnified on a cachectic face. But his spirit seems valiant as ever, which sends me scrambling to wonder when we had discussed this impending trip, how it slipped my mind, and most importantly, why I had not encouraged it well before these final days of his life.
A flight from Melbourne to Sydney perhaps. Easy and short. Or further maybe, to Alice Springs – difficult but not impossible. Several times I have stopped palliative chemotherapy to honour a patient’s wish to take a trip.
“Where are you flying?” I ask.
“Asia.” he says, and I do a double-take. “They have curative treatment there.”
I should have guessed.
“There is this famous hospital where they give special therapy to kill cancers that have stopped responding to chemo. They sound amazing.”
Every oncologist spends time drawing a distinction between useful adjunctive therapies including reflection, meditation and exercise and dangerous extreme alternatives like exclusion diets and vitamin overdoses, but judging by his tone I calculate that my time would be more wisely spent trying a different approach.
“I am worried about you deteriorating while overseas in a country that has poor hospitals and no palliative care services. I’d hate for you to be stuck”
“I’ve spoken to them, they can fix me,” he says.
“They can’t fix you,” I gently respond. “I know this is really difficult but stay here and let us help you. At least give it some thought.”
Brandishing a manila envelope, he says, “The flight is booked, we leave tomorrow.”
Many retorts, pleas, and memories of misadventure cross my mind, still I hold my tongue, understanding that the measure of grief and the promise of hope amount to much more than the weight of my frustration.
“Doctor,” says my patient. “You have nothing further to offer me, please don’t block my way.”
We arrive at the impasse we had to have.
“I won’t change your mind but I can’t declare you fit to fly,” I say.
At this, I think of the times I have been called to assist ill patients on long-haul flights. Many were emergencies but some not. An elderly lady had felt unwell throughout that day’s dialysis and subsequently suffered an arrest on the plane. “Who cleared her to travel?” I plaintively asked her husband as she drifted in and out of consciousness.
Her situation had stressed hundreds of passengers, distracted the pilot, and put a nurse and me in the impossible situation of resuscitating a patient with bare resources and deafening noise.
I regard my desperate patient with something of my own desperation as I ponder my duty of care. Is it to my patient, reliant on me for a final morsel of hope? Or to all the unseen travellers who may be inconvenienced if by chance he falls ill on the flight?
To temper my pessimism, I remind myself of the grateful patients who didn’t succumb to my dire predictions. The breathless Greek patient who had lived his entire life in Melbourne but who got hold of oxygen and begged to die on home soil. The grandmother who decided that the only way she could make amends to her estranged daughter was to embrace her grandchildren who lived in Egypt. The patient who braved a trip to India by ingesting extra morphine and whose wife wrote to say his final weeks with his whole family had been the most consoling.
This man’s reasons were different but who was I to be impatient around, and judgmental about, people whose decisions departed from mine? So with my patient watching I write the most honest letter I can. It states his wish to seek treatment in a foreign country, my opinion that patients like him can deteriorate unexpectedly, and my sincere hope that he remains safe. He deems the letter fair; his family is clearly displeased.
I feel rattled until I hear that the flight was uneventful. But then the heartache continues because the treatment centre “took one look at him and told him to turn around and go back home”. Which he manages to do before plunging into further decline and succumbing to his illness a short time later in a trajectory that had been predicted.
In the ensuing months the family resists all contact, perhaps feeling angry and let down by all the people who failed their loved one. Meanwhile, the team, too, lacks closure and feels inadequate at not being able to prevent preventable suffering at the end of life.
We muse that perhaps the hardship would have felt worse had they not pursued this last avenue of hope. And maybe the only thing left to give a vulnerable patient is the gift of autonomy. These and other thoughts swirl in my mind, no doubt to be tested in the case of another patient and another patient after that, with every outcome testing and unsettling in its own way.
So many advances in cancer, so many protocols, but still missing is the protocol that says, dispense just this much fact, mix just so much optimism, offer precisely this much warning, infuse just so much hope and things will turn out fine.
For doctors, it’s about how to stand up to – and stand by – our patients to give them the very best of medicine but shield them from the worst. For patients – when to question their own discussions and when to place their trust in ours.
On many days, this seems to be the impossible quest.
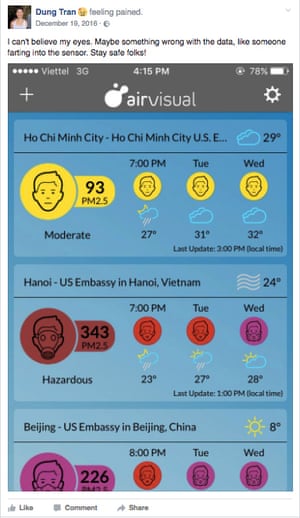
From his high-rise office building in Hanoi, Tran Dung can barely see his city’s skyline behind the thick layer of smog. Before leaving work, the 25-year-old executive assistant checks the pollution reading on his AirVisual app, which provides real-time measurements of PM2.5 – the tiny particles found in smog that can damage your throat and lungs.
Hanoi’s PM2.5 levels typically range from 100 to 200 micrograms per cubic metre – regularly within the globally acknowledged “unhealthy” category. But on 19 December last year, they hit “hazardous levels” at 343μg/m3, which was higher than Beijing.
Shocked by this reading, Dung shared a screenshot with his friends on Facebook, writing: “I can’t believe my eyes. Stay safe folks!”
He’s aware of the limitations of air quality data, which can vary between different parts of the city, but apps like this are the best tools he has.
According to the independent data measurement site AQIVN, there were at least 15 days in 2016 where average PM2.5 levels in Hanoi were “hazardous”, at 300μg/m3 or higher. On 5 October last year Hanoi had the worst air pollution among major cities across the world, generating widespread outcry over public health.
Dinh Nam, a lecturer at the Vietnam National University in Hanoi, does not need an app to tell him that the air quality is bad. “Every day I motorbike over 8km to get to work,” he says. “I can see the smog sitting on my clothing and my skin every night.”
Hanoi was measured at 343 μg/m3 of PM2.5s in December. Photograph: airvisual
Nam moved to Duong Noi, a new urban area far from the city centre, four years ago hoping to escape the pollution and traffic that the dense centre brings. However, as Hanoi continues its aggressive expansion policy, smog has caught up to his family; the area, which is close to the Yen Nghia industrial zone, has seen a simultaneous boom in high-rise construction and industrial development. The fumes from motorbike exhausts, construction and industry have made breathing a source of fear for Nam’s family. Aside from flimsy face masks, he has no other means to protect himself and his children.
When Hanoi joined a growing group of global cities to launch its first bus rapid transit route on the last day of 2016, it should have been good news for Nam. It was hoped that the new BRT would take some of the 5 million motorbikes and scooters off the roads and reduce congestion and pollution in the city.
Despite now having a BRT stop 500 metres from his house, Dinh Nam remains skeptical of the $ 53.6m development, funded by loans from the World Bank. “When the project was initiated 10 years ago, this area was much less congested than it is now. Now, the roads are so crowded it can’t be effective,” he says.
Dinh Nam’s skepticism represents the backlash BRT has faced in Vietnamese media since its launch. Many are angry that the BRT’s exclusive lane takes up almost half of some roads, exacerbating congestion for other motorbikes and cars. Others have predicted that BRT would never achieve the promise to cut travel time in half, given the challenges faced by keeping the lane free. But long before the launch, questions were already raised on whether the loan would be worth it.
The media’s declaration that BRT was dead upon arrival indicates declining trust towards the government’s handling of environmental and infrastructural challenges.
An ongoing struggle
Despite the brouhaha, many have already incorporated BRT into their daily routine. The 5pm bus towards Kim Ma on Thursday had all of its seats occupied and a handful of people standing. A dozen more gathered behind the shiny automated doors at the Giang Vo station, waiting to get in.
An official report from Hanoi’s transport document concluded that BRT passengers had risen over 62% in the first 12 days of its launch, averaging 41 passengers per trip. However, this means BRT is still operating under capacity, as can hold up to 90. Furthermore, it seems most passengers are students or retirees who are probably already accustomed to using public transport.
Given the low adoption, it is still too early to say whether BRT will have a positive impact on Hanoi’s air quality. The average monthly PM2.5 reading for January 2017, calculated using historical data collected at the US embassy directly on the BRT route, even shows an uptick in air pollution compared with December. However, it could be to do with the changing traffic patterns during the Vietnamese new year at the end of January.
Hanoi BRT passengers have been mainly students and the elderly who already use public transport. Photograph: Zung Nguyen for the Guardian
Dr Hoang Xuan Co, an expert at the Research Centre for Environmental Monitoring and Modelling in Hanoi, says: “In theory, implementing BRT should improve air quality by reducing the amount of private transportation. However, there are ongoing challenges with implementing BRT: the infrastructure in Vietnam is still incomplete [for example, there are no hard dividers between the BRT lane and the regular street], and people’s transportation habits are unchanged. It has been almost one month, the people have yet to see BRT really impacting air quality.”
Hanoi currently has a declining 1.3 million daily bus users, a small number in comparison to the millions of motorbike drivers. The city also has a growing appetite for cars. It is worrying that many motorbike drivers who live within the BRT route and are highly critical of its construction say they have not even considered trying it.
Motorbike culture has engrained a need for flexibility and control in many Hanoians – some do not even get off their bikes when picking up meat and produce at wet markets. Dinh Nam is afraid that transitioning to BRT would reduce his flexibility in taking care of his family. “BRT is not for me because I sometimes have to pick up my kids,” he says.
Nguyen Dung, meanwhile, avoids the BRT as she does not want to walk to and from the bus stop.
Vu Anh Tuan, director of the Vietnamese-German Transport Research Centre, believes BRT faces the challenge of promoting public transport in a motorbike and car culture.
“BRT is a wise investment because it can complement the planned metro system to form routes throughout the city, while keeping costs low. Its impact needs to be assessed by what the entire public transit network can do in the long term,” he writes in a passionate Facebook post.
“The media … will cause people to develop false perceptions about public transportation, especially BRT.”
It seems Hanoi’s new BRT system will only be able to make an impact on both reducing congestion and air quality if people are willing to change their habits.
Guardian Cities is dedicating a week to exploring one of the worst preventable causes of death around the world: air pollution. Explore our coverage here and follow Guardian Cities on Twitter and Facebook to join the discussion
Among the tiniest of the premature babies slumbering in incubators at the Mirwais hospital, one bore a name chosen by hospital staff. At five days old, “Fatima” had been abandoned by her mother after being born so early that her family assumed she was destined for the grave.
Had her relatives grasped the welcome transformation unfolding at the government-run medical centre in Kandahar, the largest city in southern Afghanistan, they might have held their newborn a little tighter.
Where once children crowded three to a bed, single occupancy is now the norm. The number of nurses making the rounds among the rows of infants has doubled, and new incubator units help neonatal specialists nurture the most fragile of lives through their first, vulnerable days.
While much of the news from southern Afghanistan over the past year has been dominated by reports of Taliban advances, the creation of a new paediatric unit at Mirwais hospital has opened a new front in a different campaign: the struggle to reduce extremely high mortality rates among Afghan infants.
Luis Tello, a Spanish paediatrician seconded to the unit by the International Committee of the Red Cross (ICRC), said the expanded facilities had already helped to persuade more Afghan mothers that, with the right care, even the weakest babies might survive.
“For me, the most astonishing improvement is with [premature] newborns. Before, nobody was taking care of them,” said Tello, speaking in a ward where young children lay on crisp white sheets, mothers at their bedsides. “But we’ve managed to change people’s minds.”
The new unit, which opened in September, is housed in a former nursing clinic in the hospital grounds, converted in a year-long project funded by the ICRC. It has 186 beds, including 15 for mothers – twice the number in the old paediatric wing.
The number of incubators has risen from six to 10, while another new ward caters for children suffering from thalassemia, a hereditary, incurable blood disease prevalent in southern Afghanistan that can be ameliorated with transfusions and medication.
By reducing overcrowding, the unit has dramatically cut the risk of contagious diseases skipping between patients. Staff who might previously have had to discharge barely improved infants to make room for even sicker children can now allow everyone time to recover.
“We won’t force them to go home early,” said Dr Muhammad Sidiq, the unit’s director. “We can let them stay here until they are completely cured.”
The unit is a tangible sign of broader progress in improving infant and maternal health. In contrast to the bleak picture on the battlefield in much of Afghanistan, years of painstaking efforts by the government and donors to improve access to basic healthcare, and train community midwives to assist at births – the vast majority of which take place at home – are yielding significant results.
I’m better off than some people – they’ve lost both their legs and arms
In 2000, Afghanistan had one of the highest infant mortality rates in the world, with almost 10% of babies dying before their first birthday, according to UN data. Since the overthrow of the Taliban in 2001, the picture has changed.
According to a comprehensive health and demographic survey, published by the Afghan government in May, the nationwide mortality rate for all infants fell from 66 to 45 deaths for every 1,000 live births between 2001 and 2015. Similarly, for all children under five, the death rate per 1,000 fell to 55 from 87.
Despite these achievements, infant mortality rates still remain high in many areas, partly due to a lack of basic education about the importance of hygiene during births. Tello explained that deadly sepsis infections could result from the common practice of using a knife to cut an umbilical cord on the sole of a shoe.
Beyond Mirwais, meanwhile, large numbers of rural women have no access to even basic clinics. Some of the mothers arriving at the unit with infants swaddled in shawls had travelled hundreds of kilometres from remote areas. Escalating violence in many parts of Afghanistan has also made facilities harder to reach: a UN study published in April documented reports of 125 security incidents affecting access to healthcare in 2015, compared with 59 in 2014 and 33 in 2013.
While the fighting begins to intensify each spring in Afghanistan, paediatric illness also follows a seasonal cycle, with diarrhoea more common in the summer and pneumonia and other respiratory diseases rife in winter. Doctors have witnessed a marked increase in malnutrition this year, possibly tied to the increasing numbers of people uprooted by fighting in the south. Some of the victims have been brought to a new therapeutic feeding centre in the unit for the most severely underweight.
Making a brisk round of the new wards, checking on patients and issuing rapid-fire instructions to nurses wearing gowns and surgical masks, Tello soon encountered one of the deadliest killers. Holding up a chest x-ray from a tiny boy named Hekmatullah, he scrutinised an image of a ribcage dotted with hundreds of tiny lesions – telltale signs of miliary tuberculosis.
“He’s lucky because he has this x-ray, which is very clear for TB,” Tello said, before hurrying to the next ward, where another listless child was battling pneumococcal meningitis.
That such children can even reach Mirwais hospital reflects the shifting contours of the war in the south. At the height of the US troop surge in Afghanistan in 2010 and 2011, intense fighting in Kandahar province flooded wards and corridors with casualties bearing blast and gunshot wounds. As the vast majority of western forces withdrew ahead of a security handover in 2014, the locus of the conflict in the south shifted into neighbouring Helmand and Uruzgan provinces, which continue to provide the hospital with a steady stream of war-wounded.
In the main hospital, a 22-year-old student named Abdul Matin was undergoing treatment after losing his right arm when a mortar round crashed into his family home in the district of Marjah in Helmand province a month earlier. Sitting up in a bed near other patients lying swaddled in bandages concealing even more grievous wounds, he greeted his injury with a certain degree of resignation.
“This is the situation,” he said. “I’m better off than some people – they’ve lost both their legs and arms.”
Despite the overwhelming challenges many patients face, Tello and his colleagues are starting to offer hope for sick children that many families might once have imagined possible. Though young “Fatima” did not survive, many more Afghans may one day look back and thank the staff at Mirwais hospital for giving them a second chance when they were most in need of help.
After four days of in-patient treatment – intensive rehydration, intravenous antibiotics and two units of blood, not to mention so many blood tests that “find the vein” became an almost full-time staff pastime – I’m feeling much better. So now back at the Royal Marsden [specialist cancer treatment hospital] for blood tests ahead of what I hope will be more chemotherapy treatment on Thursday.
And good news! Blood pressure’s up and stable; platelets and white blood cells all well within safe range – so all clear for treatment. This is quite a relief, and I’m sure I’m not the only cancer patient – or physician, for that matter – who feels this, but having to miss treatments is frustrating and a bit of a worry. The fear being that as treatments are skipped, the cancer and its offshoots will regain ground, thus making them harder to treat further down the line. Anyhow, none of that this week!
Thursday 17 November
Having missed a week of treatment, whereas this should’ve been a double drug week – paclitaxel on the NHS, and ramucirumab up in the private patients’ “suite” – in fact, as we’re in what is in effect now week two in the cycle, it’s NHS paclitaxel only.
Infusion goes well – once they’d found a vein for the cannula (the rather clever device through which infusions are delivered into veins). With the cold cap applied I still live in hope that I won’t lose my hair. And what a relief to have actually got another round of treatment!
Friday 18 November
In Manchester today for an appearance on BBC Breakfast’s sofa at an outside broadcast they’re doing to mark the end of a series of reports on cancer – one of which, as I think I mentioned before, featured me and a conversation with my old friend Nick Robinson about how to discuss cancer with family, friends and the world beyond. The programme came from the Maggie’s centre at the Christie hospital. Maggie’s centres are there for people with cancer – and others affected by it: carers, family, friends etc – to drop in for help, advice or just a chat.
It was heartening to meet other people living with cancer – and a great coming-together moment when the presenter tried to tell three of us we had “terminal” cancer, which was met with a good humoured but unanimous raspberry. The only certainties in life are, as they say, death and taxes, and so it is when you’ve got cancer. I might have weeks, months, years or even a full lifespan ahead of me. I know I’ve got advanced cancer and well recognise that changes the odds considerably – but I’m not out yet and neither were any of my fellow contributors.
I was asked one question, though, which really made me think. Why had I decided to be so public about my cancer? Which as I sat in the Maggie’s centre did make me think about how privileged my position is compared with so many others with cancer diagnoses.
First, I’m a journalist and so have a way of approaching my own disease which interests and engages me as a story in its own right and – as any journalist will attest – once you’ve got a story, the urge to tell it is almost irresistible. Second, I have access to ways of telling it both on the radio and in print. And third, I’m not 35 and still building a career or in the dating game or running my own business where I’m the key business winner. Who would want to tell a prospective boss or date or client about a diagnosis like mine? Nor am I facing a relationship breakdown by revealing all – you don’t exactly make yourself an investment by telling people you’ve got cancer.
For me, by contrast, there is virtually no downside. I suppose what I’ve realised is that for many people, that’s just not the case. So there is a long way to go in terms of society in general coming to terms with the realities of cancer – after all, Cancer Research statistics suggest that one in two of us will get it at some point in our lives.
Tuesday 22 November
Back to the Marsden today for blood tests ahead of treatment on Thursday – I hope! I’ve been feeling generally OK, although pesky kidney stones have been back. Unfortunately, the tests show that my platelet count has dropped again and so has the level of the white blood cells – critically important to fighting infections.
My consultant, Dr Starling, appears even more fed up and disappointed than me, especially because there are some very early signs – no symptoms from the main tumour at all, improved liver function and other markers showing positive – that might suggest the new regime is working on the cancer. Trouble is, it might also be rendering me unable to safely receive it. Consultant wondering – but really hoping not – whether I might be in the 2% of people (yes, 2%) to whom the drug paclitaxel appears to do this. Naturally I am with her on this!
So treatment on Thursday now looking unlikely. More self-injections to promote white blood cell production prescribed, and more blood tests (we really are running out of veins) booked for early Thursday morning …
Wednesday 23 November
Up at 6.15 to prepare for The Media Show. But, to be honest, the kidney stones are killing me, the medication can make one a bit dopey, and I’m feeling pretty fatigued. So 7am speak to producer, who takes the news brilliantly well and sets out to find a stand-in presenter. I always feel bad doing this but BBC Radio has been really brilliant about it, and I guess if I did present a programme and made a hash of it I’d feel quite a lot worse.
Thursday 24 November
Back at the Marsden. Blood results not great so definitely no treatment today. Another date missed and more of the frustration and underlying issues to worry about. But a platelet infusion later and it’s onwards and upwards!
Friday 25 November
Months ago I agreed to a request from the Media Society – and the London Press Club and the Royal Television Society – to consider participating in an evening looking at my career. Flattering and hard to turn down in many ways but weirdly like an invitation to my own wake. With the help of BBC Radio they managed to get the historic Radio Theatre at Broadcasting House, home to so many BBC comedies and performances. And the event is tonight!
It is framed as an interview between me and Roger Bolton, presenter of Radio 4’s Feedback but a TV executive of many, many years’ experience who once upon a time as editor of Nationwide gave me my first proper job in telly. Well, 300 guests and a packed Radio Theatre beckoned – and, I should say, with every likelihood of a £2,000-plus donation to the Marsden charity. But what had I let myself in for?
Back at the Marsden again, the platelet count had improved but there was no significant movement on the white blood cells and the amazing Dr Starling was actively worrying about whether I should even do the Radio Theatre event. Ultimately she relents, and with a very strict set of instructions – get a cab there and back, stay away from anybody with a cough or cold, and if you get a temperature or even feel just really off, call the emergency helpline immediately – gives me her blessing.
Audience reaction was truly amazing and utterly humbling. As wakes go, it’ll be one to remember – which I trust I will for many years to come!
To donate to Maggie’s centres, visit maggiescentres.org
John McDonnell describes the last six years of economic policy as an ‘abject failure’ in the House of Commons on Wednesday. The shadow minister accuses Philip Hammond of failing the sick and elderly after his autumn statement gave no additional money to the NHS or social care
Thank you to all our Veterans. For far too long– gratitude for service, understanding the depth of emotional wounds, and lack of timely, compassionate care for the physical—have plagued our VA system.
It’s time our Veterans become educated and empowered about new and highly effective treatments for wounds both visible, and deeply hidden.
Along with the election, came the legalization of marijuana in several states. Make no mistake—we have a long way to go. This is not “pot smoking” like so many believe it to be. This is Cannabis—one of the oldest, most effective medicinal plants—showing up in government PubMed published studies with the potential to help more than a hundred ailments. New treatments from an old favorite are showing promise for everything from cancer and Alzheimer’s—to depression, diabetic neuropathy, fibromyalgia, Parkinson’s, epilepsy, MS, and pain. Herbalists and Naturopaths are rejoicing. Even allopathic physicians and caring responsible oncologists can no longer deny the science-based evidence. Why does cannabis work on so many seemingly different ailments? It has to do with the nervous system. Endocannabinoids are a group of molecules that affect neurons and their specific receptors in the brain. They have been studied extensively and found to play a part in the way the body processes appetite, pain sensation, mood and memory.
Endocannabinoids are part of the ECS (endocannabinoid system) already within us. This system maintains normal cerebral and physiological function. Any type of neurodegenerative disease will be helped by taking in exocannabinoids in the proper form to correct deficiency due to genetic issues or lifestyle choices. Endo are in us but not in the plant–exo are in the plant and when we consume Cannabis (one of the oldest medicinal plants)–we fortify our inner ECS system for good or bad depending upon which cannabis compounds we consume. The terpenes for example, inhibit amyloid plaque (anti-Alzheimer’s). Some are potent hallucinogens. So cannabis can potentiate or diminish, and negatively or positively interact with the human ECS. Responsible scientists are cultivating cannabis for the betterment of mankind—while there will always be those who exploit the plant for personal gain. Patented drugs like Marisol manipulate the natural plant extract components, which then lose the ability to work with the body to restore function. Patented drugs have side effects (in this case possible seizures) that nature does not.
Another one of my favorite innovations from Jorg C. Gerlach of the McGown Inst. For Regenerative Medicine, is the Skin Gun. This allows severe burn patients to use their own skin stem cells to heal in merely days; helps avoid infection, and painful, grafting procedures. Healing the physical wounds in a timely and minimally painful way is important for beginning the process of inner emotional healing.
Companies utilizing 3D printers to make prosthetics that are both realistic looking and fully functioning should be available to all Veterans– along with the physical therapy to fully restore activities of daily living. Integrating back into a meaningful life purpose prevents isolation and depression.
Evox Therapy is another cutting edge treatment for healing the mind. Every physical ailment begins as a perception of an event filtered by the mind. You must address the emotional component to heal the physical. This is not accomplished with drugs. Drugs suppress this process, not heal it. Evox therapy is a perception reframing therapy using the frequency of your voice to release negative energy. Biofeedback allows patients to receive helpful frequencies based upon their targeted vocal recognition to unblock and release toxic stressors and reframe perceptions with healing positive energy. (Links in resources)
There is a privately funded, non-profit healing center in Bluemont, Virginia where natural healing therapies are successfully treating PTSD. The “Warrior Path” program is 18 months long and teaches people how to leave the past behind and find a new center for personal growth. Natural effective therapies include things like hiking, fishing, culinary skills, bonfires, music, and even a Labyrinth. (Links below)
This Veteran’s Day, let’s honor our heroes by empowering them back from helplessness and despair to health beyond danger —body, mind, and Spirit.
Resources:
Cannabis—one study http://medical-cannabis-declaration.org/jahan-marcu/
At the end of a 20km red dirt track winding through a rainforest in eastern Paraguay, lies a secondary school for girls providing a source of hope in a country that has a notorious reputation when it comes to women’s rights.
“Machismo is very strong here,” says Palmira Mereles, as she scrapes the dirt from a freshly unearthed root vegetable, a manioc, in the school’s garden. “Only men have a voice. Women aren’t encouraged to have dreams or opinions.”
Now 21, Mereles was part of the first year group to study at the Mbaracayú Education Center when it opened in 2009. Built by the NGO Fundación Paraguaya, it aims to tackle precisely the problems she points to: the issues of gender equality in this small landlocked country.
It has been a year since Paraguay’s strict abortion laws were brought to international attention when a 10-year-old girl was denied a termination. The girl, known as “Mainumby”, was allegedly raped by her stepfather, but abortion in the predominantly Catholic country is only legal if the mother’s life is at risk. Amnesty International describes these laws as “draconian”, and despite repeated requests from the girl’s mother, protests within the country and across the world, the authorities refused to allow it.
We were treated like a house of witches
This was not an isolated incident. Teen pregnancy rates are among the highest in the region. More than one in 20 girls under 20 have given birth (pdf); and in rural areas, like the Atlantic forest, a quarter of these girls are aged 14 or under. As a result, many are unable to finish their education.
“Gender discrimination is common across Paraguay,” says Celsa Acosta, the school’s founding director. “Poverty is desperate, particularly in rural areas, and girls suffer the worst consequences. We wanted to help them take control of their own lives.”
Protests against child sexual abuse erupted in Asuncion, Paraguay’s capital, after the Mainumby case. Photograph: Cesar Olmedo/AP
Activists have often come up against the country’s traditional Catholic background. Gloria Rubín who was Paraguay’s minister for women when the school was built, produced a sex education handbook to be distributed to Paraguayan secondary schools. But the church organised protests against it, and the book was withdrawn. When she later travelled around teaching the handbook directly to teachers across Paraguay, the church pursued her with demonstrations, she says. “We were treated like a house of witches.”
[Sex education] is taught from the perspective of the Catholic church, which means it’s stuck in the 19th century
The school sits in an isolated clearing surrounded by the Mbaracayú reserve, which protects the largest surviving fragment of Atlantic forest in Paraguay (only 7% of the original forest remains). The small campus is scattered with dormitories, classrooms and thickets of lofty palms. Alongside the vegetable garden where they grow potatoes, maize, courgettes and peanuts, there’s a livestock farm, hotel rooms, and a tourist trail winding into the undergrowth.
In this richly fertile yet vulnerable area, the school aims to grow these girls into leaders of sustainable development in their communities. They are taught techniques for agribusinesses and IT skills, which is particularly unique for indigenous communities. Alongside the national curriculum, they can also study a range of vocations, including textiles, tourism and environmental management. More radically, they provide programmes on gender, self-esteem, and sex education.
Sex education across the country is “inadequate” according to Rubín. “It’s taught from the perspective of the Catholic church, which means it’s stuck in the 19th century,” she says. Yet it has a central role at the Mbaracayú school. Girls are taught about their sexual and reproductive rights on a weekly basis, in what the school describes as “orientation” classes focusing on their physical and psychological health.
The Atlantic forest is home to the only living examples of almost 10,000 species of plant. Photograph: Felipe Dana/AP
“I became pregnant very young, because I lacked the information to know any better,” school founder Acosta explains. “It really marked me as a person. I decided then to make sure girls of the next generation have access to the information that I never did.
“We teach about contraception and ensure girls understand their own fertility,” she continues. “But just as important, in a macho culture, is cultivating their self-esteem. They need to know what they want and be able to assert it in their relationships.”
The school also gives a second chance to girls who previously dropped out of education. Elva Gomez, 19, lives and studies here with her four-year-old daughter.
“Before coming here, I thought I’d just stay at home and look after Romina,” she says. “But now I want to finish my studies and train to be a nurse.”
The Mbaracayú school hopes that girls will be able to better support themselves and their families with the qualifications and skills they offer. Students from indigenous communities study for free, while most Paraguayan families pay 100,000 guaraní a month (£12). And though many parents of local indigenous communities were initially sceptical about this progressive school, most are now keen for their daughters to study there after witnessing its benefits – two graduates of the 2011 class are now primary school teachers in their communities.
Students are also encouraged to apply for university scholarships, both within the country and abroad. Mereles studied agricultural sciences in Costa Rica, before returning to teach and run the vegetable garden.
“I’ve known many girls who didn’t want to continue studying,” she says. “They didn’t believe they could achieve anything. But over time their attitudes change. They become much more confident.”
With the school’s drop out rate at just 9% compared to 17% throughout the region, there is a new generation of girls from the heart of the Mbaracayú forest who are gaining the confidence to fight for their rights – and the potential for change in the rest of the country is perhaps within reach.
Join our community of development professionals and humanitarians. Follow @GuardianGDP on Twitter. Follow the conversation on the hashtag #LatAmNow.
I entered the field of mental health social work just a few weeks ago, joining a psychosis team. I had been warned by friends, family, taxi drivers and the media that this area of work is in dire straits and suffering hugely from cuts and poor practice.
After a couple of days, I could confirm that the former is true: swingeing cuts have had a drastic effect. Therapeutic groups and the time practitioners are able to spend with service users are incredibly stretched, and diaries no longer set aside any time for breaks – or, it seems, any time to breathe. However, my observations of current practice contradict the tales of woe.
I spent one day with a mental health support worker, shadowing him on four home visits with service users, and I was touched by the remarkable work he is doing. In the car between visits, we spoke about the value of things like listening, getting fresh air, and working collaboratively with each service user.
I had come across words like “collaborative” and “active listening” time and again in literature and legislation on mental health practice, but had pessimistically assumed that, for the most part, this language served to tick boxes for inspectors.
The support worker valued the time spent with each service user as much as they did with him
Here, I witnessed these things being practised in the truest, most genuine sense. The support worker valued the time spent with each service user as much as they did with him, and I observed them continuously teaching and learning from one another.
This was not in an expensive psychiatric unit or over a £4 coffee, but simply during walks, exploring new areas and the changing seasons, discovering the best places to go. It occurred to me that so much essential work, even administrative obligations, could take place in these settings. Why not?
Understanding of what good practice means is changing, and mental health finally seems to be taking centre stage in public discourse.
Unfortunately, because these changes have taken place in the era of austerity, many ideas about the value of a social approach feel unfeasible in practice. As a result, a return to a medical model is tempting, and can seem like the most time-saving and cost-effective option. However, from what I have seen, expensive medication with often complex side effects, compares poorly with therapeutic support.
Medication is undeniably an important part of recovery for some service users, but the knowledge that they have been prescribed drugs to alter their thoughts automatically places them in a category of “in need”, or in some sense “less human”.
The social work I have observed is therapeutic input at its best. Despite the challenges ahead – inevitable in every job – I am so grateful that the negative attitudes towards the field of mental healthcare are being challenged and contradicted in daily practice. Workers, such as the people I’ve met, are not giving up hope, and as a result, service users are not giving up hope either. This, to me, is the greatest outcome we could wish for.
The Social Life Blog is written by people who work in or use social care services. If you’d like to write for the series, email socialcare@theguardian.com with your ideas.
Join the Social Care Network to read more pieces like this. Follow us on Twitter (@GdnSocialCare) and like us on Facebook to keep up with the latest social care news and views.
Scientists are finalising plans to use gene therapy to treat one of the world’s most widespread inherited diseases – sickle cell anaemia. The technique could begin trials next year, say researchers.
About 300,000 babies are born globally with sickle cell disease. The condition causes red blood cells to deform, triggering anaemia, pain, organ failure, tissue damage, strokes and heart attacks. In the west, patients now live to their 40s thanks to the availability of blood transfusions and other treatments. But in Africa most still die in childhood.
“We have known exactly what is the cause of sickle cell anaemia for 60 years, but it has been enormously difficult to turn that information into a treatment,” said Prof Stuart Orkin of Harvard Medical School. “There are a million steps between the lab bench and the clinic, it turns out. However, I think we are closer.”
Sickle cell anaemia is triggered by a genetic fault that changes one of the dozens of amino acids that make up haemoglobin, the key constituent of the red blood cells that carry oxygen around our bodies. The mutated haemoglobin undergoes a change in shape and blocks veins.
The condition is carried by symptomless parents and is thought to have arisen in Africa, the Caribbean and other areas as a protection against malaria. However, when two carriers have children there is a one-in-four risk a child will inherit two sickle cell genes, one from each parent, and develop the disease. In Britain a screening service is offered to parents. Nevertheless more than 300 affected children are born every year.
Crucially, not every person with sickle cell disease succumbs to the condition, scientists have found. Some appear to be protected against its ravages. “We have two types of haemoglobin,” explained Orkin. “There is foetal haemoglobin whose production is normally switched off when we are born. Then the standard adult version takes over.”
But in some individuals foetal haemoglobin production is not turned off at birth. “Those individuals are supplied with foetal haemoglobin throughout their lives and for those who also inherit sickle cell anaemia this protects them against the disease by making a substance that can carry oxygen round the bodies,” he said. “We have calculated that you only need to make a small amount of foetal haemoglobin to halt sickle’s symptoms.”
The prospect of boosted foetal haemoglobin levels in patients was helped when it was found that a gene called BCL11A acts as a suppressor of foetal haemoglobin production. “Essentially, it switches off foetal haemoglobin’s manufacture after birth,” said Orkin. “What we aim to do is to stop it doing this. We want to suppress the suppressor and allow foetal haemoglobin to continue to be made in the body.” And crucial to this task was the discovery by Orkin and colleagues that a small piece of the BCL11A gene, called the enhancer, controls foetal haemoglobin expression.
“We can now use gene-editing technologies to cut out that little enhancer so that the BCL11A gene stops shutting down foetal haemoglobin production and allow children with sickle cell disease to start making it in their blood,” added Orkin. “Essentially, we will take bone marrow – where blood cells are made – from a patient, gene-edit it so that those cells produce enhanced levels of foetal haemoglobin, and return them to that patient.”
Orkin said the science had now been worked out. “We hope to begin trials in the near future.” He added that several other centres in the US were gearing up to start gene therapy trials for sickle cell using similar approaches.
David Williams, of the Boston Children’s Cancer and Blood Disorders Center, is using a slightly different technique to boost foetal haemoglobin but also hopes to begin trials next year. “When you knock BCL11A down, you simultaneously increase foetal haemoglobin and repress sickling haemoglobin, which is why we think this is the best approach,” said Williams.
Such treatments were only like to help patients in the west, Orkin acknowledged. “What we need is a pill that will boost foetal haemoglobin in patients, one that is simple to administer,” he said. “That is our ultimate goal, and the lessons we learn from our gene therapy work will help us get there. Once we do that we can then say we have conquered sickle cell.”