Electroconvulsive therapy is such a serious treatment that there is something almost prosaic about the place where it happens. There is a sense that the therapy is no more dramatic – or time-consuming – than visiting a blood bank. There is even a tea and biscuit station at the end.
Within a suite of five rooms at the Barnet, Enfield and Haringey Mental Health NHS trust, classical music floats across the airwaves casting an uplifting atmosphere over the standard hospital decor of blue lino, magnolia walls and no-nonsense chairs.
Robert Tobiansky, the lead ECT consultant, talks us through a typical procedure.
“We treat anywhere between 30 and 50 patients per year and it has been like that for as long as I have been around,” he says, adding that numbers for the clinic, held twice a week, vary throughout the year. “Our list today was five – we have been very busy lately.”
The ECT machine. Photograph: Linda Nylind for the Guardian
We pass through a small waiting room and then an office-like space where each patient is talked through the process of ECT and asked for their consent.
Next is the treatment room, a clinical space with one trolley bearing anaesthetic equipment and another carrying the ECT machine.
“It might not look like much, but that blue box cost 25 grand,” says Tobianksy. He picks up the electrodes, or paddles – each about the size of a coffee jar – and demonstrates how they are placed on a patient’s head.
The machine is also connected to what appears to be a jumble of cables. These, says Tobiansky, are for monitoring the patient’s brain activity throughout the procedure. “As well as being able to give an electric stimulus, in such a way that it is giving minimal amounts of electricity but sufficient to induce a seizure, it also monitors the duration of the seizure,” he explains.
After lying down on a trolley the patient is given an anaesthetic and muscle relaxant, with blood oxygen and heart rate monitored. The paddles are then placed on their head and a current applied for just a few seconds – inducing a short seizure.
A stint in the recovery room follows – an airy space with four beds each bearing a green mattress and yellow pillow. On the walls are paintings, while blue blinds are half drawn at the window.
The recovery room. Photograph: Linda Nylind for the Guardian
Typically, says Tobiansky, patients are a little groggy, perhaps with a headache or nausea as they come round. “We check how quickly people become re-oriented by asking: ‘Do you know where you are? Do you know the date?’ etc, and we are documenting how long that takes.” Within 15 minutes most patients are back on their feet.
The final room contains a kettle – patients are offered tea or coffee and a biscuit before they leave the suite, an important step since the general anaesthetic means they have had to fast for six hours prior to the treatment.
Typically, says Tobiansky, ECT is used to treat patients with severe depression, often accompanied by psychotic symptoms, a high risk of suicide or a refusal to eat or drink.
“This is somebody who through their depression feels that they are not worthy of eating or drinking, who through their illness is starving – that is a life-threatening condition,” says Tobiansky. “You have not got time to wait for other things not to work. Likely things have been tried and failed.”
But, he adds, negative, dramatic depictions of the treatment in film and other media have left their mark. “Although it is small numbers of people who have the treatment we usually have a big battle against the stigmas and the very negative press ECT has,” he says.
While Tobiansky admits ECT can cause memory problems, and it is difficult to predict to what degree that will affect each patient, he says there is no evidence that it causes brain damage or dementia.
“I have seen it help so many people over so many years where nothing else has helped them,” said Tobiansky.
“In my opinion, ECT is underused. [But] it is not a panacea.”
A private mental healthcare clinic that treated celebrity patients such as Lily Allen, Johnny Depp and Amy Winehouse has been ordered to make improvements amid concerns for the safety of patients at risk of suicide or self-harm.
The Priory hospital, in Roehampton, south-west London, is occupying a Grade II-listed building and is known as Priory Healthcare group’s “first and most well-known hospital”.
The hospital is best known for treating celebrities, particularly for drug addiction, and has been described as the British equivalent of the Betty Ford Clinic in the US.
The list of well-known patients includes songwriter Pete Doherty, former footballer Paul Gascoigne and Lloyds Banking Group chief executive António Horta-Osório.
The Priory treats a wide range of mental health problems including depression, anxiety and addictions. Some of the facilities on offer to private patients include an on-site restaurant, a gym with a personal trainer and housekeeping for a number of the private en-suite rooms.
But the Care Quality Commission (CQC) gave the hospital a rating of “requires improvement” following an inspection. The regulator issued the provider with a warning notice after inspectors rated the hospital as “inadequate” for providing safe care.
But Priory Healthcare, which runs the hospital, said it was “disappointed” the regulator decided to re-inspect its facility in the middle of a £1.2m improvement programme.
The CQC argued that the hospital was not providing safe levels of staffing to meet the needs of their patients.
The inspection report reads: “There remained high vacancy rates for nurses across the hospital and particularly on the eating disorder service. This resulted in high use of bank and agency staff and there were also a significant number of shifts with below safe staffing levels.
“Records indicated that there were more incidents on shifts with insufficient staff on Priory Court, the eating disorders unit for children and adolescents. There had been 95 incidents on Priory Court in the six months prior to the inspection.
“Following the inspection the provider sent us revised figures indicating a higher level of staffing than indicated at the time of the inspection. We undertook enforcement action against the provider, serving a warning notice regarding staffing levels.”
The regulator launched a re-inspection of the premises in October last year after it highlighted concerns during a visit in March 2016.
It said that in addition to concerns about staffing levels, inspectors concluded that the hospital environment, particularly on the acute wards, remained unsafe for patients at risk of suicide or self-harm.
Inspectors rated the trust as “good” for being effective and caring but “requires improvement” on being responsive.
Dr Paul Lelliott, the CQC’s deputy chief inspector for mental health, said: “When we inspected the Priory Hospital in October 2016, we were very concerned about the safety of patients at risk of suicide or self-harm.
“The hospital must ensure it can meet the needs of patients they choose to admit whilst improvements to staffing and the environment take place.
“We did however find some improvements and noted that the provider had implemented a pre-admission risk assessment.
“The wards also provided a comprehensive range of psychological therapies, including dialectical behavioural therapy, mindfulness, and family therapy. Occupational therapists and dietitians facilitated activities and discussion groups.”
Commenting on the inspection, Dr Sylvia Tang, chief executive of Priory Healthcare, said: “Roehampton is a safe hospital providing high quality care and treatment and we remain fully committed to making improvements for the benefit of all of our patients.
“Our £1.2m improvement programme at Roehampton is being led by a new management team and includes trialling a state-of-the-art patient monitoring system.
“It is disappointing that we have been re-inspected part-way through this programme when there were works in progress which have now been completed.
“Similarly, we question CQC’s findings in relation to staffing: our rotas show that appropriate staff-patient ratios have been maintained and, over the last year, we have reduced the vacancy rate for nurses by more than 50%, despite a national shortage of nurses.”
In the UK, the Samaritans can be contacted on 116 123. In the US, the National Suicide Prevention Hotline is 1-800-273-8255. In Australia, the crisis support service Lifeline is on 13 11 14.
A London clinic for women who have undergone FGM is being forced to close after the local council withdrew funding from March 2017.
The Acton African Well Woman Centre was awarded the Guardian sponsored Diversity and equality award in 2011 and houses experts in the field of female genital mutilation (FGM) who are able to help women who have have been through the trauma of the procedure.
The facts you should know about female genital mutilation
It also offers women de-infibulation – a reversal of of the most extreme form of FGM. Type III is the removal of the entire genitalia, leaving a hole small enough for urine and menstrual blood to pass through.
“Ealing council’s priority is to raise awareness of FGM and the support available to a wider audience,” a spokesman told the Guardian.
“We will continue to commission FGM awareness work in the borough to reach more people such as schools and community groups and signpost women to clinical support,” he added.
The clinic was notified of the council’s decision late last year, but the closure was confirmed following the rejection of a last-ditch appeal to Ealing Clinical Commissioning Group for alternative funding.
Staff have told the Guardian closing the clinic will destroy a strong community of women who bring, “sisters, cousins and friends” to the service.
“I don’t think anyone is questioning the value and expertise of the service,” a worker said, but I wonder if it was white middle class women who were vocal and out there would they close down the service?
“These are vulnerable women and they don’t have many places to go. It’s devastating that this clinic can’t survive after 10 years demonstrating that it is a goal standard.”
Since opening in 2007, the Acton clinic has seen more than 1,000 women in its fortnightly open hours and staff have performed upwards of 500 de-infibulations.
A number of healthcare professionals have been trained by the clinic, including GPs at a community-based service in Bristol, which is modelled on the Acton service.
The clinic does not refuse women from outside Ealing borough, which means any woman from across the UK can walk in. Women have come from as far as Northern Ireland seeking help.
Psychotherapist, survivor, and campaigner Leyla Hussein has referred women to the clinic. “What commissioners need to understand is that there’s a taboo,” she said. “[Women] aren’t going to go to the clinic in their area and we shouldn’t put barriers around them when they need to have access. I’m shocked and disappointed that the commissioners didn’t take that into account.
“A majority of women are cut by women. The idea of these of women trusting other women is a big deal. That they trust them is brave of these women to do that. Now that they have become confident and trusting, it’s going to be taken away from them.”
A petition to save the service has gathered over 11,000 signatures.
The NHS has been accused of letting down patients in pain by shutting London’s last community-based A&E-style service for people needing emergency dental treatment.
NHS England’s closure of the “urgent dental service” in Kentish Town will leave the capital’s 8.7 million residents with only two busy hospitals to go to with teeth problems. Dentists have warned that it will force more patients to seek help at overcrowded GP surgeries and A&E units. The disappearance is the latest loss of walk-in services across England for people with emergencies such as a broken tooth or abscess.
NHS England said the service would shut on 31 March, even though 5,451 people used it last year and patients come from all over London to get treatment. People should in future call the NHS111 helpline or seek an appointment with their regular dentist, they said.
“Access to emergency dental care is increasingly a postcode lottery. Inadequate provision is simply piling more pressure on GPs and A&Es that are not equipped to provide dental treatment”, said Henrik Overgaard-Nielsen of the British Dental Association.
“It’s absurd that NHS111 operators are asking patients to do ring-rounds [of dental surgeries looking for a free slot at short notice],” he said.
The association is urging the NHS to tackle the growing shortage of emergency dental services by arranging for high-street dentists to always have a certain number of emergency appointments available.
“It is irresponsible to shut a fantastic service that provides emergency dental care to patients without providing an alternative. Where do they think these patients are going to go?” said Dr Francesca Silman, a doctor whose practice is near the closing walk-in centre. “It is not acceptable to leave people in pain and in need of treatment, and this will only worsen the pressures already on GPs and A&E who can offer very little help to those that attend.”
Andrew Dismore, a Labour member of the London Assembly, has voiced concern about the service going, NHS England’s lack of public consultation, and the fact that it has been taken “against the wishes” of Whittington Health, the NHS trust that staffs it.
The dental association recently estimated that 135,000 dental patients a year end up attending A&E because they cannot easily gain access to care for a sudden problem. A further 600,000 seek treatment from a GP, adding to the pressure on family doctor services, it believes.
Guy’s limits emergency dental treatment to 55 patients a day. Photograph: Frank Baron for the Guardian
From April, Londoners needing urgent dental care will have only two options: specialist clinics at King’s College Hospital and Guy’s Hospital, both in south London, though the Guy’s service limits treatment to 55 patients a day and those needing care must be there as early as 7.30am to secure an appointment. The Royal London Hospital in east London recently shut its clinic.
An NHS England spokeswoman said: “We recently reviewed the service and found that there is sufficient capacity for patients who need urgent dental care at existing dental practices and so the closure of the service would not negatively impact patients in the area.
“There are more than 1,250 high-street dentists across London where patients can access dental care when they need it. Londoners in need of urgent dental care should call NHS111, who can then signpost them to the most appropriate service for their treatment.”
Nearly 33 million Americans – more than 10% of the country’s population – have no health insurance. While the very poorest are entitled to Medicaid coverage, millions more narrowly fail to qualify, but remain too poor to pay for private health insurance. Among those who do qualify for subsidised plans or manage to pay insurance contributions, paying for minor treatments such as fillings and eye tests is often a problem, as they may not be covered by basic healthcare plans. Even finding local doctors who accept Medicaid can be so challenging that it can seem easier just to work through the pain or to self-medicate.
Virginia is one of 19 states refusing federal dollars to close the healthcare “coverage gap” for people not poor enough for Medicaid, but too poor for anything else. Yet at the Wise County Fairgrounds in Southwest Virginia, for one late-July weekend each year, there is a small glimmer of hope. For three days, a non-profit organisation known as Remote Area Medical (RAM) builds a pop-up clinic – the largest of its kind in the US – from the ground up, and serves more than 2,000 patients from more than 15 different states. These patients come in the hope of getting cavities filled, lungs x-rayed and new pairs of glasses made – for free.
RAM was founded in 1985 by Stan Brock, a British philanthropist, actor, author, naturalist, cowboy and former TV host. The organisation is funded entirely via private donations and – except for a small, paid staff – completely dependent upon thousands of volunteers for everything from performing oral surgery to making up bags of Cheerios to hand out to patients’ toddlers. In addition to international and disaster-relief missions, the group has held more than 800 general health-clinic events across 12 states throughout the southern and south-western United States. In the past five or six years, it has added urban stops such as Los Angeles and Chicago to its regular locations.
As I pull up to the Wise County Fairgrounds clinic this summer, dozens of rows of cars glint in the sun – patients’ vehicles in one field, volunteers’ in another. Those seeking care are given entry numbers based on the order in which they arrive, and cannot leave without forfeiting their place. Many make plans to camp out for up to two days before the gates even open – sleeping in their cars, in tents, or on the ground, to make sure they snag a low number.
By 3.30am on Friday,volunteers with torches are moving from car to tent to car in the patient lot, handing out admission numbers for the day. By the time the sun rises at 6am, they have given out 1,600 tickets to the clinic. On Saturday morning, they will give out about 600 more.
I meet Sheila Harris, a 58-year-old former paralegal, in the early hours of the opening day. Sheila has worked her whole life, but after the birth of the last two of her six children, steady legal work dried up, and she now earns only a small income taking care of children in her home. She is one of the first hundred people allowed through the gates. Hundreds more are packed outside the fairgrounds’ fences, waiting to hear their numbers announced via megaphone.
A woman receives dental care at the Wise County RAM clinic. Photograph: Dawn Whitmore
Sheila, her daughter Amy, her sister Cindy, Cindy’s daughter Elizabeth, and four other family members have travelled for three hours to arrive at Wise two days early. These eight adults and one toddler would end up sleeping in their two cars for four days. During the first couple of nights, they would drape blankets over the windows for privacy, but would take them down after it made the cars too hot to sit in, much less sleep.
It is everyone’s first time at the clinic, except for Cindy, who has been twice before and led the group on this trip. Once, she says, she arrived early enough to be the very first patient served. “It was still a long couple days, though,” she says.
Cindy is here this year to get new glasses and to support her 29-year-old daughter Elizabeth, who also needs glasses, as well as the extraction of two molars. Elizabeth also hopes to get a partial denture plate. She had a bad fall a couple of years ago and broke her top front teeth, most of which have been completely missing for years. At the time of her fall, she had decent health insurance, but still had to pay $ 1,000 from her own pocket, to rebuild just one tooth, which later cracked again anyway. Cindy and Elizabeth now both receive disability benefits – essentially their only source of income. Without RAM, a new pair of glasses with a current prescription would be a luxury item.
Sheila needs glasses, too, but is first set to have six teeth removed – a couple of which are already in pieces – and upper dentures made and fitted. Neither Sheila nor Elizabeth will smile open-mouthed. They haven’t smiled that way for years, out of embarrassment. “I guess I’ve kind of withdrawn from people because of it,” Sheila says. “I used to talk to anyone, anywhere, about anything – real outgoing – but I haven’t been like that in a long time.”
Sheila pulls a roll of Tums antacid tablets from her shorts pocket and says it’s the only thing she’s been able to eat since the day before, on account of her nerves. She’s brought the broken dental crown with her “in case they can use it or something”, and holds it tightly.
It is cool outside before sunrise,but the temperature will reach a humid 35C by late morning, and get even hotter by Saturday. The site has no air-conditioned spaces, apart from the mammogram and radiology trucks. Volunteers drive back and forth across the grounds all day, handing out cold water and chilled neck wraps.
Though traffic through the medical stations is steady, the main attractions of every RAM clinic are the dental and eye-care services. At the Wise County Fairgrounds, the organisation sets up about 80 mobile dental stations under large tents – one section of tents reserved for cleanings by hygienists, a second block for fillings, and, in the back tent, four or five long rows of stations for extractions. The vision and medical services are each delivered in two large barns. The makeshift examination rooms are livestock stalls, with bedsheets hung for privacy.
Stan Brock. founder of the RAM clinic, watching the operation in Wise County. Photograph: Paul J. Richards/AFP/Getty Images
The full Wise County clinic footprint is immense: one general-support volunteer working as a patient escort could easily walk 15 miles or more in a day. Specialised services such as x-rays, mammograms, and orthopaedics are provided in converted lorries or large camper vans. Other tents, offering treatment for substance abuse, counselling to help smokers quit, and mental healthcare, as well as clothing and book donations and a pharmacy, are scattered wide across the grounds. The only bathrooms – for patients and volunteers – are several dozen portaloos.
Other such RAM clinics may be smaller, but they operate under similar conditions. One in Smyth County, Virginia, is set up on the asphalt and in the emptied hangars of the local airport. Services there must shut down at a particular time so that planes can be moved back inside. One Tennessee clinic is held right on the Bristol Motor Speedway infield, a famous Nascar racing track; Stan Brock can often be seen on the track on his bicycle, vigorously pedalling angled laps.
“Poor teeth, I knew, beget not just shamebut more poorness,” writes Sarah Smarsh in her 2014 Aeon essay on class and dental hygiene. One woman sitting near Sheila and her family in Extraction Row says she has recently been fired from a waitressing job after losing a couple of her front teeth. Her manager didn’t want her in front of customers. Food service has made up the entirety of her employment history, and she is having trouble getting hired permanently elsewhere for similar reasons. Even when she was working, she says, she couldn’t afford the cost or time off necessary to treat her teeth – or anything else, for that matter. The RAM clinic, once a year, is her sole source of healthcare. She now works as a temp in one of the many call centres planted in Southwest Virginia.
Dr Joe Smiddy, one of the long-time volunteer doctors on site, has seen similar scenarios play out for patients here, time and again: “Once they lose their teeth, or they have unsightly teeth, they lose part of their own marketability. They have trouble finding a job,” he says. “Course, when they lose their job, they lose any healthcare they might have had. And then you can have substance issues where people are self‑medicating with tobacco and street drugs for what is real pain and real anxiety.”
Poverty also begets limited choices. Sugar provides a cheap and legal high and caffeine does the same. Both can be used to self-medicate and as an easy way to make your kids happy when you can’t afford much else.
Nearly 100,000 people in Southwest Virginia receive Supplemental Nutrition Assistance Program benefits (formerly known as “food stamps”). A family of four receives $ 115 per week on average for food, or just about $ 16 per day. “The economics of this community,” says Terry Dickinson, executive director of the Virginia Dental Association, “are such that when they go to the grocery store and buy food, it so happens they get a lot more food when they buy highly processed, high-carbohydrate foods, and, instead of water, they pick soda pop or sports drinks, or any of that stuff that’s just as cheap.”
Unhealthy processed foods are not just cheaper: they do not spoil as quickly, and they can take less time and fewer ingredients to prepare. “What you want for everyone is personal responsibility,” says Dickinson, “but you’ve got to give people the education and tools they need to make those decisions.” And, he says, for people living in poverty, “we just haven’t done a good job of that. These are people in survival mode.”
Living in survival mode means prioritising where you spend your limited income. A 2015 survey conducted by the Federal Reserve Board to determine what practical effects, if any, the economic recovery was having on families, found that 46% of Americans did not have enough money on hand to cover an unexpected $ 400 expense. When that expense is a medical emergency, it often leaves only two options: use a credit card if you have one, or forgo care until the pain goes well past emergency and becomes unbearable.
Putting stock in a long-term investment such as one’s health requires hope. Embedded in preventative and rehabilitative care is the presumption of a long, fulfilling life. Health insurance is an invisible protection – it does not fill a hungry stomach, or power a refrigerator, or fill a petrol tank.
Sheila is in Dr Dan Laskin’s dental chair and is about to have her extractions done. There are picks, forceps, syringes and what looks like a hammer and small chisel on the tray beside her. Even when you’re having six teeth pulled, if your dental care is happening under a tent at a fairground, you are given some numbing lidocaine, a few large, well-placed shots of novocaine, and not much more of an anaesthetic cushion than that.
The procedure is probably as smooth as it could be, though Sheila often moans and wriggles from the pressure. The dental assistant gets her to close her eyes and talks her through some visualisation strategies involving her favourite place: the beach. It takes about 30 to 45 minutes before the procedure is finished, and the experts are ready for whoever is next in line. Numbed and frazzled, Sheila says to Laskin through the packed gauze, “You are freaking amazing!” and hugs him.
Elizabeth has already had her two extractions done, and is now at the dentures station, where another dentist has inserted a tray of paste into her mouth that will become the mould used to make her partial plate. The dentist has to keep the tray pressed tight against Elizabeth’s swollen, sore jaw for about a minute. Afterwards, she says she didn’t mind it too much: “It was easier than getting my teeth yanked out!” She heads over to the vision section to get in the long line for glasses.
Observing the makeshift clinic, it sometimes feels more like a carnival than a hospital. Occasionally, in between seeing patients, you can catch Joe Smiddy picking a banjo in the clinic bluegrass band he has pulled together with a few regular volunteers. Smiddy is a 74-year-old retired pulmonary specialist, now a full-time medical volunteer, who grew up in Wise County, the grandson of a coal miner. He got his commercial driver’s licence in order to drive the 18-wheeler that holds his mobile x-ray office to RAM clinics. Smiddy has seen it all: most of what he has to share with me begins with “And I can say this because I’m from here.”
Many of the facilities at RAM clinics are housed in specially adapted trailers, lorries and vans. Photograph: Dawn Whitmore
“The people of Southwest Virginia,” he advises me, “are self-reliant, and their self-reliance and their love for their people and their land is such a wonderful thing, but it’s also what holds them here. There’s a social importance to people who are from here being really glued here. So why would we move to another part of Virginia? Why wouldn’t we move to where the jobs are? But we’re totally averse to doing that, and so we have a large population who live in an economically deprived area. The schools are struggling. The churches are struggling. Every time they build a Walmart, it puts several mom-and-pop stores out of business. Your barbershop’s gone because you get your hair cut at Walmart, your beauty salon, your auto-repair – everything Walmart. And then you’ve got people working at Walmart who don’t have health insurance, either.”
People not in poverty often ask those who are to move in various ways – off street corners when they’re homeless, away from their depressed hometowns when they’re unemployed. They are asked to move couches, off front porches and cars, off blocks.Politically, they are usually asked to move out of their own way.
All of the qualities that Smiddy describes, though, are what most people would probably say they want in a healthy community. We want people to love and care about their land and neighbourhoods and to know one another. We want a shared history, vibrant cooperation. These are all characteristics we celebrate, it seems, everywhere but communities of poverty. In places like Southwest Virginia, we do not honour these relationships, or underwrite them – socially or financially – in the same way we do in middle-class or affluent regions. Instead, what we reinforce, as a matter of policy and entertainment, are the rural stereotypes.
In his mobile rig, Smiddy will x-ray “just about anything you can put in front of the machine”. He mostly looks at lungs, though. “We’re a belt of lung disease,” he says. “Southwest Virginia is a belt of asthma, COPD [chronic obstructive pulmonary disease], emphysema, and, of course, heart attacks, strokes, and diabetes. Part of that is smoking – we in Southwest Virginia have a tradition of starting smoking at an early age. There are towns where the average age of starting smoking for current lung patients was age 10.”
But part of it, he says, is the coal dust and environmental allergens. When business was booming, coal workers were paid well and offered decent health insurance, but layoffs and closures have left many in the region with poor health, and poorer prospects for work and the healthcare coverage that used to come with it.
“All of the politicians are singing this little fairytale that coal is coming back,” Smiddy says. “They’re living in that fairytale, and so what they’re not doing is accepting the reality that we could plan, we could think ahead. We could reach broadly to incorporate everybody – schools, churches, civic organisations, mayors, community leaders – that we all pull back together and say, ‘We have a goal, and our goal is that we’re going to try to predict as best as we can the jobs of the future, and we’re going to start now.’ I don’t mean to be ugly when I say that there may be some people who will miss that curve, but we could build for their children.”
Coal is complicated in Appalachia, the mountainous region within which Southwest Virginia sits. The coal industry has torn up pieces of Southwest Virginia and the bodies of those who have mined it, but as it has declined here, the men and women it employed – many of whom have at most graduated high-school – have slipped from relying on steady middle- and upper-income salaries to prospecting for minimum wage. The classified ads in places such as Wise and Coeburn, Virginia, are thin and advertise for such positions as “Customer Service Representative 1” and “Cashier (Part Time)”. We may be able to replace coal with other comparable energy sources, but we have not yet prioritised how to comparably replace coal jobs.
“I mean, how many call centres can you put down here?” Dickinson says. All people want here, he repeats, is a good-paying job.
By Saturday, all eight of Sheila Harris’s family have spent four days and three nights living in two cars. They have had to stay this long to wait for their glasses and partial dentures to be finished.
Cindy and Amy walk over to a large tent where a few thousand brand-new frames – all donated – are set out on long folding tables so that patients can select the styles they like. A few regular volunteers consult on shape and fit.
The barn where the sight tests are given is a touch cooler than outside, mostly because the room has to be kept dark for the testing. The majority of patients here are getting basic checkups and prescriptions written or updated, but occasionally – as with the dentists – the optometrists diagnose more serious health issues: glaucoma, cataracts, macular degeneration, diabetes. Prior to their eye tests, some patients don’t even realise they need glasses.
Dr Victoria Molnar Weiss is the optometrist who runs all the Virginia RAM vision clinics. Weiss and the other eight or nine volunteer optometrists and ophthalmologists will see one third of the 2,200 patients coming through the Wise clinic over the weekend. She explains that the possibility of getting new glasses can be the lure that first brings patients to the clinics, and then, over time, their trust grows. “The patients see us up at 3am too, so it kind of helps them feel like we’re all in this together,” she says.
What also helps is the ability to use the money they might otherwise have spent on frames, lenses, and an eye test on other necessities. People living in poverty are often playing a losing game with whatever limited income they have: skipping a power bill to pay for a visit to the optician might work for a month, but it could put them behind for a year. Much easier to keep using old lenses, squint a little harder, and live through the migraines.
Elizabeth’s partial plate is finally ready. The dental technician is fitting it for her, taking it in and out of her mouth in between filing her teeth down to eventually arrive at the best fit. After a few revisions, they are both satisfied. The technician does not have a mirror, but holds up her iPhone with a forward-facing camera so Elizabeth can see herself. She has front teeth for the first time in years. She smiles and tries not to at the same time. She is now crying. Her mother, Cindy, is crying. The dental technician and I are both crying as we watch mother and daughter cry and hug each other. Elizabeth even hugs me. “It doesn’t feel normal to smile. It feels weird,” she says.
By Saturday evening, the whole family has got just about everything they came for: glasses, extractions, dentures, and even a few bags of clothes and shoes from the donations tent. They are nearly packed up when Sheila discovers her van will not start. She seems much less worried than I would be. This has happened multiple times before – she knows how to fix it herself, she says. She crawls underneath the van and reattaches a loose wire, and when she tries it, the engine turns over.
Late on Sunday morning, I catch up with Sister Bernie Kenny of the Medical Missionaries of Mary just as the clinic is closing down. Sister Bernie is a nurse-practitioner who first persuaded Stan Brock to bring RAM to Virginia back in 1999. “Today we had a young woman, 27 years old, who had all her teeth out,” she says straight away, before I can say a word past “Hello”. “And her hope for dentures is 2018. How can she live? How can her self-esteem, or her nutrition, or her hope of ever getting a job? It saddens me. But the wonder of being here is all these volunteers with one purpose: to help one another. All denominations, all faiths, all colours, everybody together, and we get energy one from another.”
Clients wait their turn to see dentists and medics. Photograph: Dawn Whitmore
I ask her what she would do if I gave her a magic wand that she could wave and change one thing for the patients here at RAM. She gives a version of the same answer that all the nurses and doctors and most of the patients give when I ask them: “Everybody has the right to healthcare – it’s not a privilege,” she says. “Your neighbour’s health affects you, so you want the best for your neighbour as well as yourself.”
Sister Bernie, like all the nurses and doctors and patients, says that dental and vision coverage need to be included in basic healthcare policies. Consider this: someone living in poverty with no health insurance gets a toothache, but swallows the pain for months. She finally goes to ER when it gets too bad to eat, sleep, or work. She sees a nurse or a doctor, but not a dentist, so the actual cause of the pain stays untreated. The ER doctor gives her some antibiotics and maybe some prescription pain medications. She uses up the prescription and then maybe looks for something cheaper on the street to dull the pain, because the tooth is never fixed. No one I speak to mentions heroin or methamphetamine by name – it’s always just “street drugs”. In the meantime, the abscessed tooth could go septic and turn just as deadly as an overdose.
Sister Bernie sees this repeatedly, across generations of families. “But the people who come to RAM want to be healthy,” she says. “A lot of them don’t take vacations, or can’t. They come here.” One patient I met started off from her house two days before the clinic opened. She had walked 27 miles to Wise just to have a couple teeth pulled. Then walked 27 miles back.
Access to healthcare is about more than just reducing the travel time between patients and doctors – it’s about bringing down those intangible barriers that make a distance seem impossible to cross. The stereotypes that teach that people living in poverty get what they deserve, the employment barriers that leave medical and dental students with a mortgage worth of school debt, such that they cannot afford to treat people who cannot afford to come to them for care. RAM does not solve and will not solve the US healthcare crisis – or poverty, for that matter – but it clears a path. One that starts right in our own backyards.
This article is adapted from an essay published in the autumn 2016 issue of the Virginia Quarterly Review.
• Follow the Long Read on Twitter at @gdnlongread, or sign up to the long read weekly email here.
Maybe you have decided that you want to open your own physical therapy clinic to help others. This is something that on one hand is relatively easy to do, but like any other business, there are downsides. You can’t just open a clinic and expect it to be filled with people and the money to just be rolling in. You really do have to work at it just like any other business if you truly want it to succeed. If you have decided that this is something you want to do, here are some tips to help get you on your way.
1. Start Out Slowly
If you have just completed your physical therapist training program, it is a good idea to work in the industry for a little while before opening your own clinic. Grow your experience at other clinics, and grow a following. Then, when you are ready to start your own clinic, you will have people lining up.
2. Learn how to be Confrontational
This probably goes against everything you learned during your training program. But, in order to be successful in business, you can’t be the type who lets others walk all over you. You need to learn how to be a leader, and how to say “no” when you have to. Learn how to deal with constructive criticism, but also know when you need to give it.
3. Treat Your Studio Like a Business
Your clinic will be a legitimate business, and you want it to make money for you. So, you need to treat it like a real business. Yes, you probably have a passion for physical therapy and want to share, but remember, if you offer too much for free aren’t going to make any money, and you are going to devalue your service.
4. Create Your Brand
Your brand, or your corporate identity, is important. It is the combination of what people see and the reputation that you earn as a business person. Your brand should combine your clinic name, the location of your clinic, logos and colors, and of course, the high quality of the service you are offering.
5. Don’t Expect Instant Riches
Most business do not make much money in the first year of operation, and this can particularly be said of physical therapy clinic. This is not a way to get rich quick. You will have to invest a lot of money to get started, for such things as space, equipment, instructors, etc. You won’t show an instant profit, but with hard work and dedication, you will succeed.
6. Learn how to be a People Person
You will need to learn more skills for dealing with people, because you are the face of your business, and people will want to talk to you about it.
7. Learn Financial Responsibility
It can be difficult to go overboard when starting a business, and you end up spending so much money that you can never dig the business out of a hole to show a profit. Don’t go out and hire a huge staff right away, or rent the largest clinic space. Do what you can afford to do now, and build from there. Over time, you will achieve the success you really desire.
For many women living in Sudan, breast cancer means certain death. Treatment is too expensive or they simply feel too embarrassed to seek help.
But until recently, yet another obstacle was seriously hampering efforts to cut breast cancer deaths in Sudan. Since the early 1990s, the country has been on the US blacklist for state sponsors of terrorism – imposed for human rights violations and for harbouring Osama Bin Laden.
Even the Khartoum Breast Care Centre (KBCC), the Horn of Africa’s first and only dedicated breast cancer clinic, has been hit by the sanctions, with a ban on international money transfers and the restriction on imports of medical equipment and spare parts.
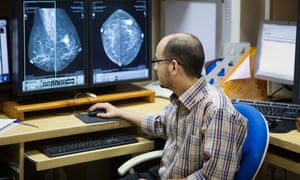
Founded by British-trained Sudanese radiologist Dr Hania Fadl, the KBCC offers hi-tech digital mammography screening for a fraction of the usual price elsewhere. Since it opened in 2010, it has treated more the 18,000 patients from across the region and has received widespread acclaim and international support.
Using private funds and a $ 14m donation from the charitable foundation run by her ex-husband, Sudanese-British businessman Mo Ibrahim, Fadl has managed its 11-year development from start to finish.
However, the US sanctions meant the centre was unable to buy and maintain crucial diagnostic machinery. In February 2014, it decided to begin a year-long application process for a US Office of Foreign Assets Control (Ofac) exemption, which would make it easier to maintain its General Electric digital mammography machine.
Dr David Lawis, medical director of KBCC. Photograph: Yassir Bukhari/Elephant Media
During the application process the machine broke down. It ended up being out of action for 10 weeks. The clinic was paralysed, with doctors forced to use alternative screening methods. “The problem is the poor women. You do ultrasounds and biopsies but an ultrasound is not an internationally approved screening modality,” Fadl says. “There are patients and I have to do something, even if they’ll put me in jail. I can’t let them wait and risk that their cancers spread.”
After heavy campaigning and several trips to Washington by Fadl to meet members of Congress, Ofac eventually issued a blanket licence exempting all medical equipment in Sudan from sanctions.
Ignorance is rife and I really hope and pray that women will come to the centre at least for a simple check up
The result was a welcome surprise to doctors at the KBCC, who say the move is a milestone for Sudanese healthcare in that it has put the needs of patients above international politics.
“All of our equipment in the clinic is from a US company, General Electric, as are the majority of advanced medical machines in Sudan. For there to be an exemption from sanctions, our lives as doctors will be much easier and the lives our patients will drastically change,” says Dr David Lawis, medical director of the KBCC.
Lawis says access to radiotherapy remains a huge issue, with just two machines in the country. One, in Khartoum a hospital, has been broken for about seven months. The second is in Madani hospital, two hours’ drive from Khartoum.
Anyone who can afford to pay for treatment abroad usually leaves Sudan to get radiotherapy, but the blanket Ofac licence has the potential to change this. “People won’t have to leave their country to get the treatment they deserve,” says Lawis.
Word of mouth
Other challenges remain, however, and Fadl says the battle to educate and inform women about self-examination and the local availability of affordable treatment is the next healthcare frontier.
“We did a little survey to ask the women how they heard about us. We found that the most effective, at 49%, was word of mouth. We are still a tribal community: we trust relatives, friends and neighbours who tell us ‘I went to that place and it is good’. We don’t have that culture of research on the internet,” says Fadl.
This was the case for 60-year-old Sudanese patient Fatma Abdelmajid, who regularly takes a six-hour bus from Atbara in north-east Sudan to Khartoum for treatment after a local doctor told her that “one of Atbara’s boys” worked at the KBCC clinic.
Women wait to be seen at the KBCC. Photograph: Yassir Bukhari/Elephant Media
“The mentality around breast cancer here is absolutely wrong. When you tell women in the village that you’ve been diagnosed, they are so disturbed as if you’re about to drop dead in front of them. It’s really sad,” says Abdelmajid.
“They tell you, go to a fakeeh [spiritual healer], who will give you herbs and spiritual remedies to treat you. Ignorance is rife and I really hope and pray that women will come to the centre at least for a simple checkup.”
While the Sudanese health ministry keeps no full records, Lawis says that breast cancer accounts for approximately 35% of all cancer cases among Sudanese women. An estimated 60% of the 2,000 women diagnosed with breast cancer who die each year could have survived if given proper care.
Fadl strongly believes that stories like Abdelmajid’s will help end the taboo that often stops women from seeking a diagnosis. “A woman who has the experience of being treated should tell her stories, to new patients here at the centre and women in their villages. The best thing is to have these examples and success stories,” she says.
Fadl, who lives above the centre in Khartoum, patrols the corridors every day, greeting patients. “If I just walk downstairs and see the patients, see their kindness and deep gratitude, I just can’t help but want to help them. Sudanese women deserve everything I do – really and truly. I can’t tell you enough.”
Imagine you’re a doctor in Swindon and a patient with a chewing tobacco habit turns up with unusual tongue lesions. What if you could, at the press of a few buttons, locate and get instant advice from the Mumbai-based world expert on cancers related to chewing tobacco?
This is the vision for a new app which aims to transform the way in which 8.5 million doctors around the world share their knowledge and skills.
MDLinking – an expert directory, instant messaging service and video source – began trialling a beta version for iPhones in May this year and aims to launch its full Apple and Android versions before 2017.
The Dutch startup, which has €2.5m of seed funding, has several hundred testers in the Netherlands, 4,000 registered doctors so far and is in talks with organisations including Médecins Sans Frontièresand the Aga Khan Development Network (AKDN) about using its free software.
“The original idea was that if doctors worldwide connect with each other and share knowledge, healthcare will improve on a global level” says Alec Behrens, co-founder of Booking.com and founding partner of MDLinking.
Instant messaging
Many doctors are already using instant messaging tools to discuss patient cases. A 2015 survey found more than 30% of doctors surveyed said they were sending patient related information over services such as WhatsApp.
Vascular surgeon Hans Flu, co-founder of MDLinking, came up with the idea for the secure healthcare network when he realised just how much his colleagues were using WhatsApp. He had privacy concerns over the app and worried about its plans to share account information with parent company Facebook.
Ultimately, however, Flu wants to find a solution to what he sees as the big problem in the medical world: communication. “If you communicate badly, the patient’s going to suffer, and this is a key element that everyone can improve. This is a tool developed by medical doctors, for medical doctors, that is free.”
As well as being a directory and secure instant messaging tool (it only accepts vetted medical professionals), the start-up is using virtual reality technology to record operations from multiple viewpoints, to form an interactive teaching tool – especially for countries where operating theatres are scarce.
Dr Hans Flu, co-founder of MDLinking Photograph: Hans Flu
Gijs Walraven, director for health at AKDN – which operates a non-profit, private healthcare system in developing world communities – is interested in collaborating with the MDLinking tool.
“AKDN’s work in health is mainly in sub-Saharan Africa, central and south Asia,” he says. “In these countries, there are fewer medical doctors and they have much more limited opportunities to consult with colleagues on difficult cases as well as to [access] education. New ways to interact at a distance and in a secure manner could play a very important role to improve this.
“Learning new operating techniques and how to better diagnose using the innovative video techniques that MDLinking is developing could be a real breakthrough.” And it works both ways, he says: “Healthcare providers in rural settings in Afghanistan have knowledge and skills that could be beneficial to health practitioners in London.”
Teaching by virtual reality
Dr Gijs van Acker, a surgeon at Medisch Centrum Haaglanden hospital in the Netherlands, first created teaching videos for his vascular surgery website a decade ago. “One of my residents was Hans Flu, and when he started MDLinking I said, ‘You need something that’s educational’. We wanted to make something more intuitive than 2D films,” he says.
They came up with virtual reality combined with the view-selection interface, allowing users to flick to different sections of the operation. Traditional teaching methods can’t compete, according to van Acker, who says that dead body tissue loses its colour, so isn’t the same teaching experience, while students observing actual operations are often distracted by nerves.
He has recorded four 3D operations for MDLinking so far and – thanks to a partnership providing Samsung equipment – these are viewable via mobiles and virtual reality headsets.
As the app is free, the business plans to raise revenue by broadcasting sponsored medical conference content and acting as a recruitment site for international medical placements. It wants to establish video centres in different places around the world using tools and facilities available there – for example, treating appendicitis in remote Africa.
Kiran Jobanputra, deputy head of the Manson Unit at Médecins Sans Frontières in London, says the organisation is looking into MDLinking as it develops a medical IT strategy. “Until something is piloted and evaluated, it is hard to say, but I do see potential in this app,” he says. “Having been a field doctor, I came up against huge difficulty getting access to information, particularly relevant technical advice.”
He says MSF medical experts at the London HQ and its telemedicine platform have time, context and connectivity limitations. “MSF clinicians are using WhatsApp groups of colleagues to get rapid, relevant advice – although it’s not an official MSF tool, and some people in the organisation might not agree with it,” he says. “That MDLinking ‘LinkedIn’ function to join or create a new group of people happy to give their opinion, with regional experience, has huge potential.
“I suspect the educational content will still require connectivity of too high bandwidth. We’re not testing MDLinking at the moment but if it comes on to Android, which is the main smartphone operating system in the contexts we work in, we probably will.
“The sharing economy isn’t new – in our medical studies we are taught ‘see one, do one, teach one’ – but barriers to sharing information are getting lower.”